

Pneumonia in children in the developing world: new challenges, new solutions
- PMID: 15480964
- PMCID: PMC7129317
- DOI: 10.1053/j.spid.2004.05.010
Pneumonia in children in the developing world: new challenges, new solutions
Abstract
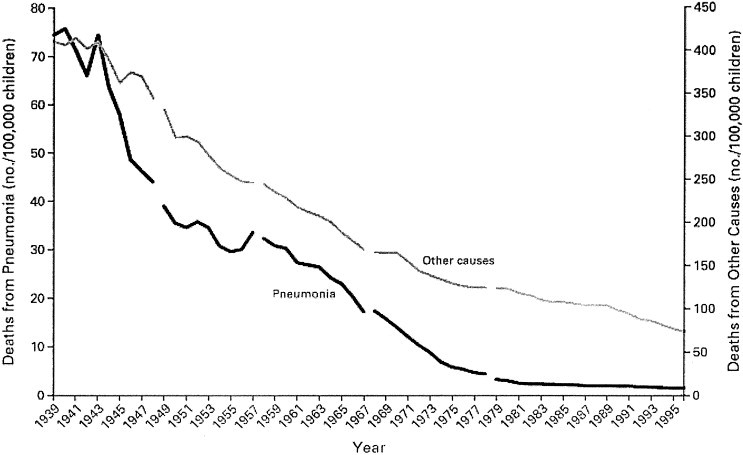
Pneumonia has been a leading cause of death in both developed and developing countries as long as health indicators have been available. Yet the issues of concern for this syndrome are far from static. Improvements in access to health services have lowered infant mortality rates, benefiting children around the world and lowering the fraction of child deaths caused by pneumonia. However, progress has been interrupted repeatedly by the emergence of new pathogens. Landmark randomized controlled trials have now demonstrated the effectiveness of Haemophilus influenzae type b (Hib) and multivalent pneumococcal conjugate vaccines against childhood pneumonia, as well as meningitis and bacteremic disease. Momentum has gathered to tackle long-standing economic obstacles to expand access to new vaccines and programs for the poorest countries of the world. A pressing challenge for the control of pneumonia in developing countries is to identify better metrics for pneumonia. Surveillance tools are needed that will bridge studies of interventions, establish preventable disease burden, and serve as indicators for monitoring new programs.
Figures

References
-
- Murray C., Lopez A. Harvard School of Public Health; Boston: 1996. Global Health Statistics: A Compendium of Incidence, Prevalence and Mortality Estimates for Over 200 Conditions.
-
- Williams B.G., Gouws E., Boschi-Pinto C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002;2:25–32. - PubMed
-
- Jones G., Steketee R.W., Black R.E. Bellagio Child Survival Study Group. How many child deaths can we prevent this year? Lancet. 2003;362:65–71. - PubMed
-
- Dowell S.F., Kupronis B.A., Zell E.R. Mortality from pneumonia in children in the United States, 1939 through 1996. N Engl J Med. 2000;342:1399–1407. - PubMed
-
- Sazawal S., Black R.E. Meta-analysis of intervention trials on case-management of pneumonia in community settings. Lancet. 1992;340:528–533. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
