

Haemodynamic effects of remifentanil in children with and without intravenous atropine. An echocardiographic study
- PMID: 15486003
- PMCID: PMC4767884
- DOI: 10.1093/bja/aeh293
Haemodynamic effects of remifentanil in children with and without intravenous atropine. An echocardiographic study
Abstract
Background: Remifentanil is known to cause bradycardia and hypotension. We aimed to characterize the haemodynamic profile of remifentanil during sevoflurane anaesthesia in children with or without atropine.
Methods: Forty children who required elective surgery received inhalational induction of anaesthesia using 8% sevoflurane. They were allocated randomly to receive either atropine, 20 microg kg(-1) (atropine group) or Ringer's lactate (control group) after 10 min of steady-state 1 MAC sevoflurane anaesthesia (baseline). Three minutes later (T0), all children received remifentanil 1 microg kg(-1) injected over a 60 s period, followed by an infusion of 0.25 microg kg(-1) min(-1) for 10 min then 0.5 microg kg(-1) min(-1) for 10 min. Haemodynamic variables and echocardiographic data were determined at baseline, T0, T5, T10, T15 and T20 min.
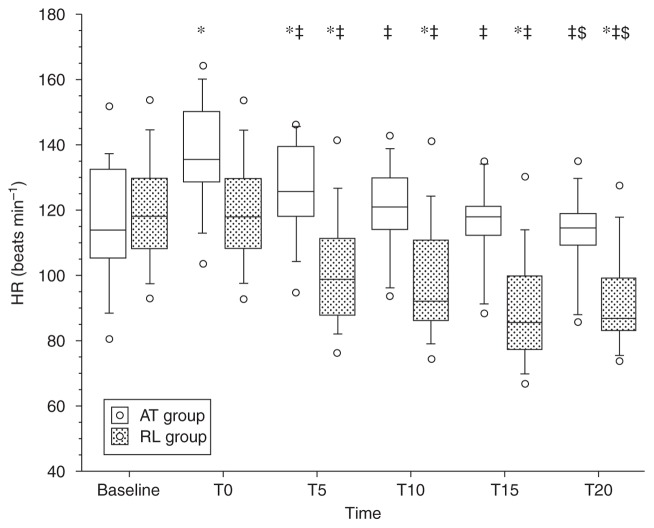
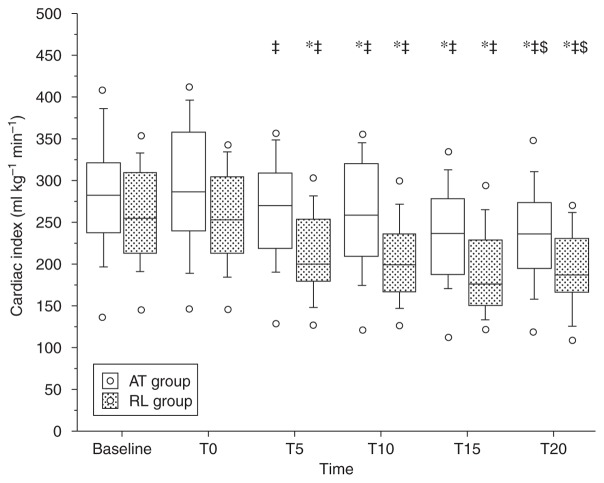
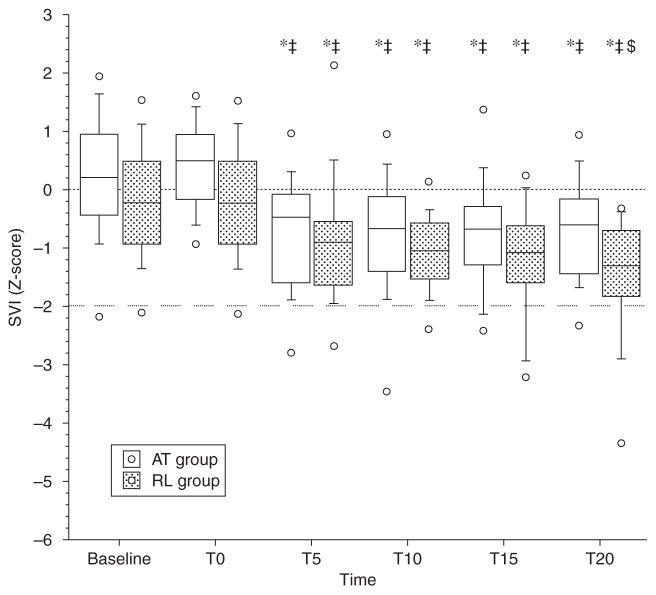
Results: Remifentanil caused a significant decrease in heart rate compared with the T0 value, which was greater at T20 than T10 in the two groups: however, the values at T10 and T20 were not significantly different from baseline in the atropine group. In comparison with T0, there was a significant fall in blood pressure in the two groups. Remifentanil caused a significant decrease in the cardiac index with or without atropine. Remifentanil did not cause variation in stroke volume (SV). In both groups, a significant increase in systemic vascular resistance occurred after administration of remifentanil. Contractility decreased significantly in the two groups, but this decrease remained moderate (between -2 and +2 sd).
Conclusion: Remifentanil produced a fall in blood pressure and cardiac index, mainly as a result of a fall in heart rate. Although atropine was able to reduce the fall in heart rate, it did not completely prevent the reduction in cardiac index.
Figures
Similar articles
-
Glycopyrrolate during sevoflurane-remifentanil-based anaesthesia for cardiac catheterization of children with congenital heart disease.Br J Anaesth. 2005 Nov;95(5):680-4. doi: 10.1093/bja/aei254. Epub 2005 Sep 30. Br J Anaesth. 2005. PMID: 16199414 Clinical Trial.
-
Cerebral haemodynamic changes during propofol-remifentanil or sevoflurane anaesthesia: transcranial Doppler study under bispectral index monitoring.Br J Anaesth. 2006 Sep;97(3):333-9. doi: 10.1093/bja/ael169. Epub 2006 Jul 7. Br J Anaesth. 2006. PMID: 16829673 Clinical Trial.
-
Effect of remifentanil with and without atropine on heart rate variability and RR interval in children.Anaesthesia. 2005 Oct;60(10):982-9. doi: 10.1111/j.1365-2044.2005.04298.x. Anaesthesia. 2005. PMID: 16179043 Clinical Trial.
-
Intraocular pressure more reduced during anesthesia with propofol than with sevoflurane: both combined with remifentanil.Acta Anaesthesiol Scand. 2002 Jul;46(6):703-6. doi: 10.1034/j.1399-6576.2002.460612.x. Acta Anaesthesiol Scand. 2002. PMID: 12059895 Clinical Trial.
-
Remifentanil; from pharmacological properties to clinical practice.Adv Exp Med Biol. 2003;523:245-60. doi: 10.1007/978-1-4419-9192-8_22. Adv Exp Med Biol. 2003. PMID: 15088856 Review. No abstract available.
Cited by
-
Estimating 'lost heart beats' rather than reductions in heart rate during the intubation of critically-ill children.PLoS One. 2014 Feb 4;9(2):e86766. doi: 10.1371/journal.pone.0086766. eCollection 2014. PLoS One. 2014. PMID: 24503645 Free PMC article.
-
Remifentanil-based total intravenous anesthesia for pediatric rigid bronchoscopy: comparison of adjuvant propofol and ketamine.Clinics (Sao Paulo). 2014 Jun;69(6):372-7. doi: 10.6061/clinics/2014(06)01. Clinics (Sao Paulo). 2014. PMID: 24964299 Free PMC article. Clinical Trial.
-
Pressure-volume loop-derived cardiac indices during dobutamine stress: a step towards understanding limitations in cardiac output in children with hypoplastic left heart syndrome.Int J Cardiol. 2017 Mar 1;230:439-446. doi: 10.1016/j.ijcard.2016.12.087. Epub 2016 Dec 22. Int J Cardiol. 2017. PMID: 28043677 Free PMC article.
-
Perioperative complications in children with pulmonary hypertension undergoing noncardiac surgery or cardiac catheterization.Anesth Analg. 2007 Mar;104(3):521-7. doi: 10.1213/01.ane.0000255732.16057.1c. Anesth Analg. 2007. PMID: 17312201 Free PMC article.
-
Hemodynamic effects of target-controlled infusion of propofol alone or in combination with a constant-rate infusion of remifentanil in dogs.Can J Vet Res. 2015 Oct;79(4):309-15. Can J Vet Res. 2015. PMID: 26424912 Free PMC article. Clinical Trial.
References
-
- Egan TD, Lemmens HJ, Fiset P, et al. Remifentanil versus alfentanil: comparative pharmacokinetics and pharmacodynamics in healthy adult male volunteers. Anesthesiology. 1996;84:821–33. - PubMed
-
- Prys-Roberts C, Lerman J, Murat I, et al. Comparison of remifentanil versus regional anaesthesia in children anaesthetised with isoflurane/nitrous oxide. International Remifentanil Paediatric Anaesthesia Study group. Anaesthesia. 2000;55:870–6. - PubMed
-
- Ross AK, Davis PJ, Dear Gd GL, et al. Pharmacokinetics of remifentanil in anesthetized pediatric patients undergoing elective surgery or diagnostic procedures. Anesth Analg. 2001;93:1393–401. - PubMed
-
- Hogue CW, Jr, Bowdle TA, O’Leary C, et al. A multicenter evaluation of total intravenous anesthesia with remifentanil and propofol for elective inpatient surgery. Anesth Analg. 1996;83:279–85. - PubMed
-
- DeSouza G, Lewis MC, TerRiet MF. Severe bradycardia after remifentanil. Anesthesiology. 1997;87:1019–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
