

Association of house spraying with suppressed levels of drug resistance in Zimbabwe
- PMID: 15491495
- PMCID: PMC535889
- DOI: 10.1186/1475-2875-3-35
Association of house spraying with suppressed levels of drug resistance in Zimbabwe
Abstract
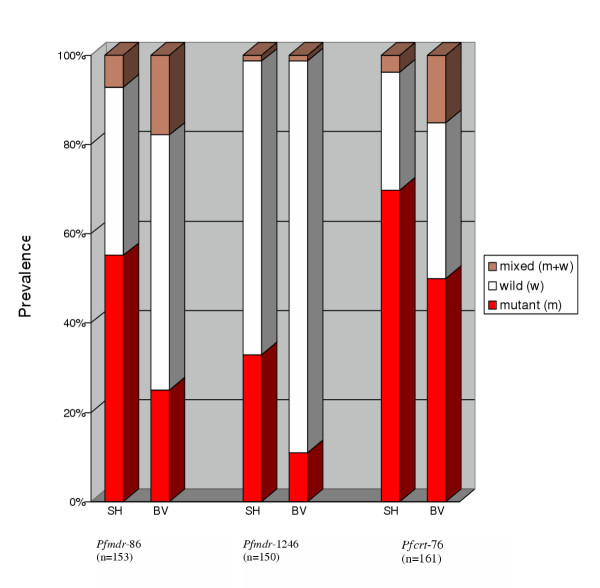
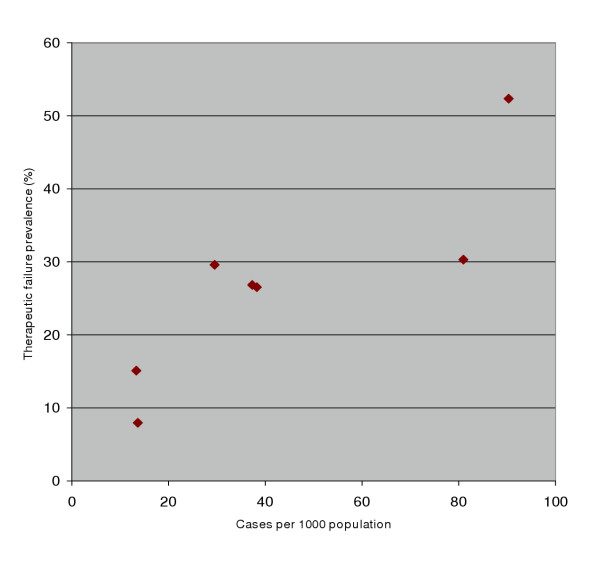
Background: Public health strategies are needed to curb antimalarial drug resistance. Theoretical argument points to an association between malaria transmission and drug resistance although field evidence remains limited. Field observations, made in Zimbabwe, on the relationship between transmission and multigenic drug resistance, typified by chloroquine, are reported here.
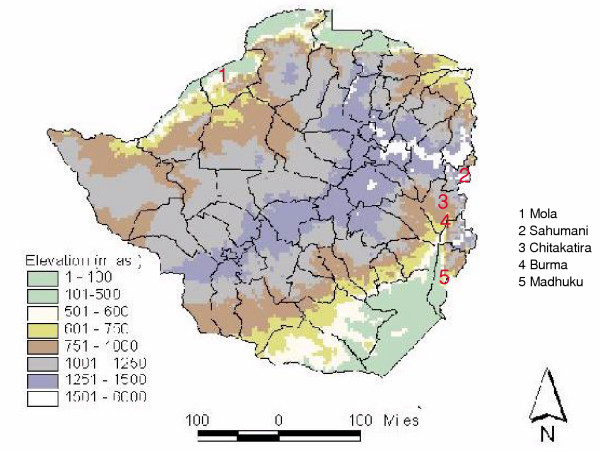
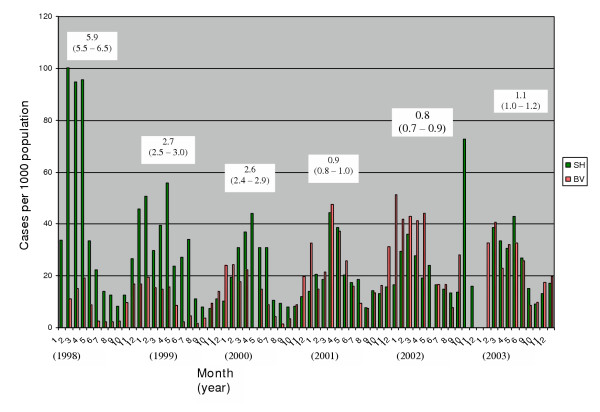
Methods: Periodic assessments of the therapeutic response of uncomplicated falciparum malaria to chloroquine in two selectively sprayed or unsprayed health centre catchments, from 1995 - 2003. Cross-sectional analysis of in vivo chloroquine failure events for five sites in relation to natural endemicity and spraying history.
Results: During selective house spraying, the chloroquine failure rate for the sprayed catchment decreased, such that, after four years, the odds of chloroquine failure were 4x lower than before start of spraying in the area (OR 0.2, 95% CI 0.07 - 0.75, p = 0.010, n = 100). Chloroquine failure odds for the sprayed area became 4x lower than contemporaneous failure odds for the unsprayed area (OR 0.2 95% CI 0.08 - 0.65, p = 0.003, n = 156), although the likelihood of failure was not significantly different for the two catchments before selective spraying started (OR 0.5, 95% CI 0.21 - 1.32; p = 0.170, n = 88). When spraying ended, in 1999, the drug failure odds for the former sprayed area increased back 4 fold by 2003 (OR 4.2, 95%CI 1.49 - 11.78, p = 0.004, n = 146). High altitude areas with naturally lower transmission exhibited a 6x lower likelihood of drug failure than low-lying areas (OR 0.16 95% CI 0.068 - 0.353, -2 log likelihood change 23.239, p < 0.001, n = 465). Compared to sites under ongoing annual spraying, areas that were last sprayed 3-7 years ago experienced a 4-fold higher probability of chloroquine failure (OR 4.1, 95%CI 1.84 - 9.14, -2 log likelihood change 13.956, p < 0.001).
Conclusion: Reduced transmission is associated with suppressed levels of resistance to chloroquine and presumably other regimens with multigenic drug resistance. It seems the adoption of transmission control alongside combination chemotherapy is a potent strategy for the future containment of drug-resistant malaria.
Figures
Similar articles
-
Contribution of the pfmdr1 gene to antimalarial drug-resistance.Acta Trop. 2005 Jun;94(3):181-90. doi: 10.1016/j.actatropica.2005.04.008. Acta Trop. 2005. PMID: 15876420 Review.
-
Plasmodium chloroquine resistance and the search for a replacement antimalarial drug.Science. 2002 Oct 4;298(5591):124-6. doi: 10.1126/science.1078167. Science. 2002. PMID: 12364789
-
High-level chloroquine resistance in Sudanese isolates of Plasmodium falciparum is associated with mutations in the chloroquine resistance transporter gene pfcrt and the multidrug resistance Gene pfmdr1.J Infect Dis. 2001 May 15;183(10):1535-8. doi: 10.1086/320195. Epub 2001 Apr 13. J Infect Dis. 2001. PMID: 11319692
-
Recovery of chloroquine sensitivity and low prevalence of the Plasmodium falciparum chloroquine resistance transporter gene mutation K76T following the discontinuance of chloroquine use in Malawi.Am J Trop Med Hyg. 2003 Apr;68(4):413-5. Am J Trop Med Hyg. 2003. PMID: 12875289
-
Conservation of a novel vacuolar transporter in Plasmodium species and its central role in chloroquine resistance of P. falciparum.Curr Opin Microbiol. 2001 Aug;4(4):415-20. doi: 10.1016/s1369-5274(00)00228-9. Curr Opin Microbiol. 2001. PMID: 11495804 Review.
Cited by
-
Changes in the burden of malaria following scale up of malaria control interventions in Mutasa District, Zimbabwe.Malar J. 2013 Jul 1;12:223. doi: 10.1186/1475-2875-12-223. Malar J. 2013. PMID: 23815862 Free PMC article.
-
Progress towards malaria elimination in Zimbabwe with special reference to the period 2003-2015.Malar J. 2017 Jul 24;16(1):295. doi: 10.1186/s12936-017-1939-0. Malar J. 2017. PMID: 28738840 Free PMC article.
-
Emergence of urban malaria and the associated risk factors: a case-control study in Mutare city, Zimbabwe.Malar J. 2025 Jul 28;24(1):245. doi: 10.1186/s12936-025-05494-4. Malar J. 2025. PMID: 40722086 Free PMC article.
-
Individual- and Household-Level Risk Factors Associated with Malaria in Mutasa District, Zimbabwe: A Serial Cross-Sectional Study.Am J Trop Med Hyg. 2016 Jul 6;95(1):133-40. doi: 10.4269/ajtmh.15-0847. Epub 2016 Apr 25. Am J Trop Med Hyg. 2016. PMID: 27114289 Free PMC article.
-
High prevalence of molecular markers for resistance to chloroquine and pyrimethamine in Plasmodium falciparum from Zimbabwe.Parasitol Res. 2007 Sep;101(4):1147-51. doi: 10.1007/s00436-007-0597-5. Epub 2007 Jun 3. Parasitol Res. 2007. PMID: 17546463
References
-
- Trape JF. The public health impact of chloroquine resistance in Africa. Am J Trop Med Hyg. 2001;64:12–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
