

Resolved and unresolved controversies in the surgical management of patients with Zollinger-Ellison syndrome
- PMID: 15492556
- PMCID: PMC1356480
- DOI: 10.1097/01.sla.0000143252.02142.3e
Resolved and unresolved controversies in the surgical management of patients with Zollinger-Ellison syndrome
Abstract
Objective: Highlight unresolved controversies in the management of Zollinger-Ellison syndrome (ZES).
Summary background data: Recent studies have resolved some of the previous controversies including the surgical cure rate in patients with and without Multiple Endocrine Neoplasia-type1 (MEN1), the biological behavior of duodenal and pancreatic gastrinomas, role of imaging studies to localize tumor, and gastrectomy to manage acid output.
Methods: Review of the literature based on computer searches in Index Medicus, Pubmed and Ovid.
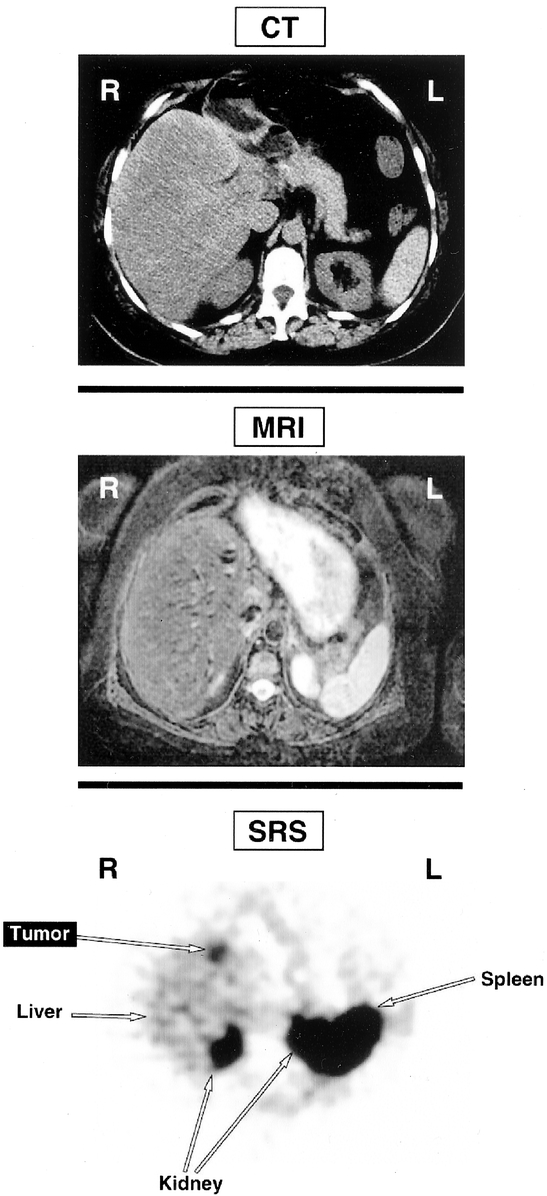
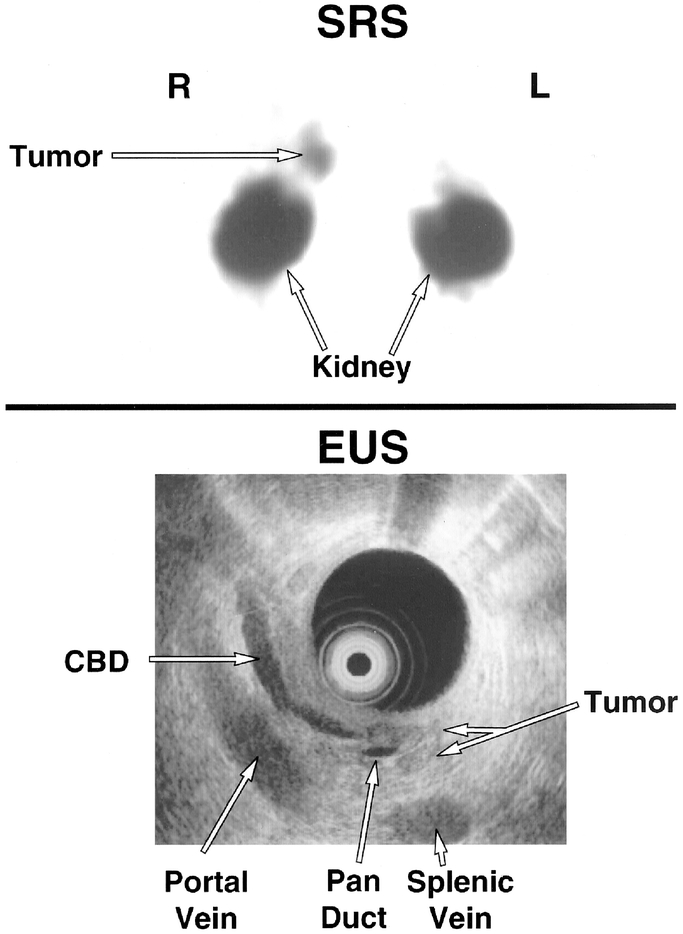
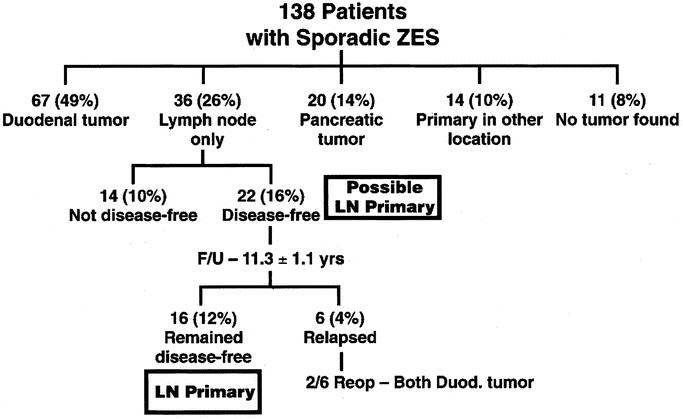
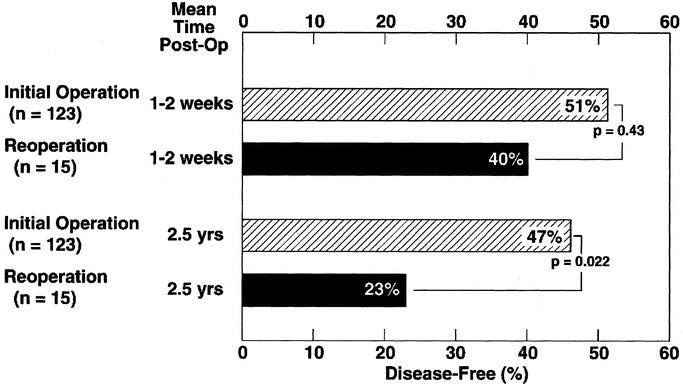
Results: Current controversies as identified in the literature include the role of endoscopic ultrasound (EUS), surgery in ZES patients with MEN1, pancreaticoduodenectomy (Whipple procedure), lymph node primary gastrinoma, parietal cell vagotomy, reoperation and surgery for metastatic tumor, and the use of minimally invasive surgical techniques to localize and remove gastrinoma.
Conclusions: It is hoped that future studies will focus on these issues to improve the surgical management of ZES patients.
Figures
References
-
- Norton JA, Jensen RT. Unresolved surgical issues in the management of patients with the Zollinger-Ellison syndrome. World J Surg. 1991;15:151–159. - PubMed
-
- Roy P, Venzon DJ, Shojamanesh H, et al. Zollinger-Ellison syndrome: clinical presentation in 261 patients. Medicine. 2000;79:379–411. - PubMed
-
- Pipeleers-Marichal M, Somers G, Willems G, et al. Gastrinomas in the duodenums of patients with multiple endocrine neoplasia type 1 and the Zollinger-Ellison syndrome. N Engl J Med. 1990;322:723–727. - PubMed
-
- vanHeerden JA, Smith SL, Miller LJ. Management of the Zollinger-Ellison syndrome in patients with multiple endocrine neoplasia type 1. Surgery. 1986;100:971–977. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
