

Meta-analysis of laparoscopic versus open pyloromyotomy
- PMID: 15492557
- PMCID: PMC1356481
- DOI: 10.1097/01.sla.0000143250.48265.d6
Meta-analysis of laparoscopic versus open pyloromyotomy
Abstract
Objective: To perform a meta-analysis of studies comparing open pyloromyotomy (OP) and laparoscopic pyloromyotomy (LP) in the treatment of infantile hypertrophic pyloric stenosis.
Background: LP has become increasingly popular for the management of pyloric stenosis. Despite a decade of experience, the real benefit of LP over the open procedure remains unclear.
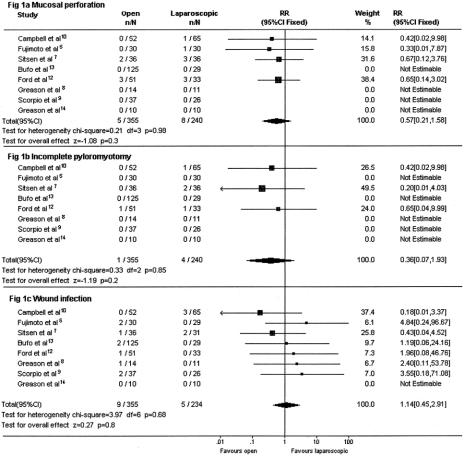
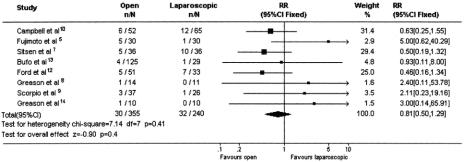
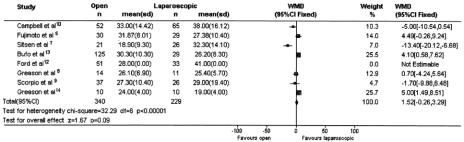
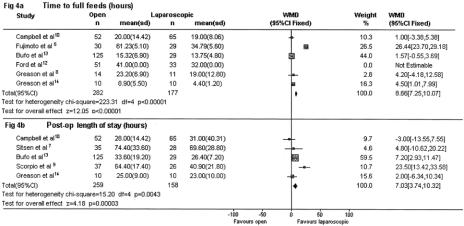
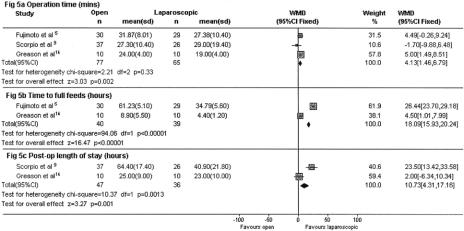
Methods: Using a defined search strategy, studies directly comparing OP with LP were identified (n = 8). Data for infants treated by both approaches were extracted and used in our meta-analysis. OP and LP were compared in terms of complications, efficacy, operating time, and recovery time. Weighted mean difference (WMD) between continuous variables and 95% confidence intervals (95% CI) were calculated. For dichotomous data, relative risk (RR) and 95% CI were determined.
Results: Only 3 studies were prospective, and just 1 study was a prospective randomized controlled trial. Mucosal perforations and incomplete pyloromyotomy were both more common with LP. Compared with OP, LP is associated with higher complication rate (RR 0.81 [0.5, 1.29], P = 0.4), similar operating time (WMD 1.52 minutes [-0.26, 3.29], P = 0.09), shorter time to full feeds (WMD 8.66 hours [7.25, 10.07], P < 0.00001), and shorter postoperative length of stay (WMD 7.03 hours [3.74, 10.32], P = 0.00003).
Conclusions: OP is associated with fewer complications and higher efficacy. Recovery time appears significantly shorter following LP. A prospective randomized controlled trial is warranted to fully investigate these and other outcome measures.
Figures
References
-
- Grant GA, McAleer JJ. Incidence of infantile hypertrophic pyloric stenosis. Lancet. 1984;1:1177. - PubMed
-
- Ramstedt C. Zur operation der angeborenen pylorus stenose. Med Klin. 1912;26:1191–1192.
-
- Alain JL, Grousseau D, Terrier G. Extramucosal pyloromyotomy by laparoscopy. Surg Endosc. 1991;5:174–175. - PubMed
-
- Tan HL, Najmaldin A. Laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis. Pediatr Surg Int. 1993;8:376–378. - PubMed
-
- Fujimoto T, Lane GJ, Segawa O, et al. Laparoscopic extramucosal pyloromyotomy versus open pyloromyotomy for infantile hypertrophic pyloric stenosis: which is better? J Pediatr Surg. 1999;34:370–372. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
