

Gastric decompression and enteral feeding through a double-lumen gastrojejunostomy tube improves outcomes after pancreaticoduodenectomy
- PMID: 15492567
- PMCID: PMC1356491
- DOI: 10.1097/01.sla.0000143299.72623.73
Gastric decompression and enteral feeding through a double-lumen gastrojejunostomy tube improves outcomes after pancreaticoduodenectomy
Abstract
Objective: The objective of this study was to assess the feasibility and safety of inserting a double-lumen gastrojejunostomy tube (GJT) after pancreaticoduodenectomy (PD) and to evaluate associated outcomes.
Background: Gastroparesis is a frequent postoperative event following PD. This often necessitates prolonged gastric decompression and nutritional support. A double-lumen GJT may be particularly useful in this situation: gastric decompression may be achieved through the gastric port without a nasogastric tube; enteral feeding may be administered through the jejunal port.
Methods: Thirty-six patients with periampullary tumors were randomized at the time of PD to insertion of GJT or to the routine care of the operating surgeon. Outcomes, including length of stay, complications, and costs, were followed prospectively.
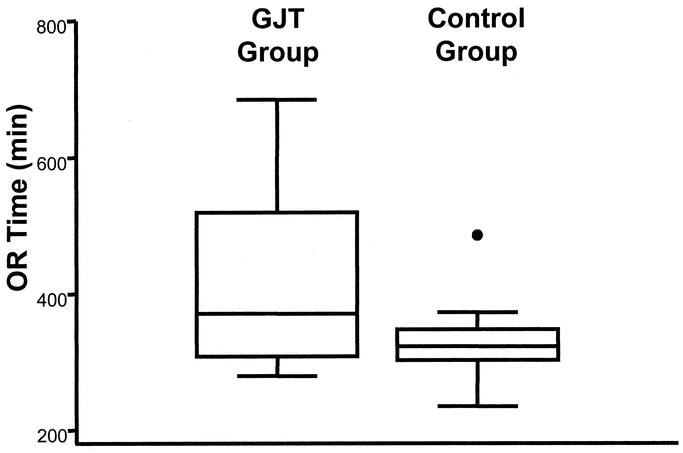
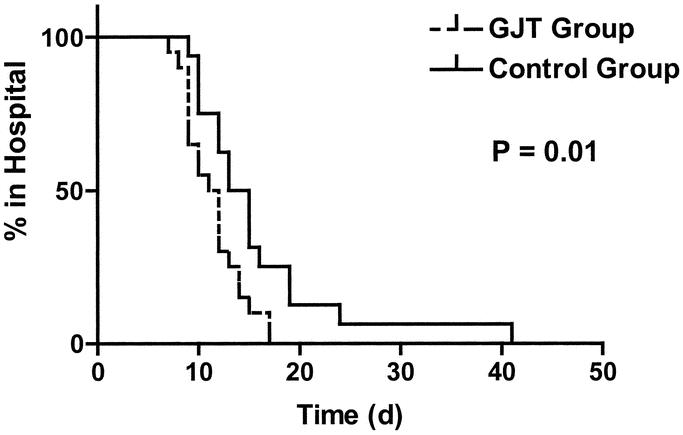
Results: The 2 groups had similar characteristics. Prolonged gastroparesis occurred in 4 controls (25%) and in none of the patients who had a GJT (P = 0.03). Complication rates were similar in each group. Mean postoperative length of stay was significantly longer in controls compared with patients who had a GJT (15.8 +/- 7.8 days versus 11.5 +/- 2.9 days, respectively; P = 0.01). Hospital charges were 82,151 +/- 56,632 dollars in controls and 52,589 +/- 15,964 dollars in the GJT group (P = 0.036).
Conclusions: In patients undergoing PD, insertion of a GJT is safe. Moreover, insertion of a GJT improves average length of stay. At the time of resection of periampullary tumors, GJT insertion should be considered, especially given this is a patient population in which weight loss and cachexia are frequent.
Figures
Similar articles
-
Enteral nutrition and biliopancreatic diversion effectively minimize impacts of gastroparesis after pancreaticoduodenectomy.J Gastrointest Surg. 2009 May;13(5):929-37. doi: 10.1007/s11605-009-0831-9. Epub 2009 Feb 18. J Gastrointest Surg. 2009. PMID: 19224292 Clinical Trial.
-
Feeding patients with preoperative symptoms of gastric outlet obstruction after pancreatoduodenectomy: Early oral or routine nasojejunal tube feeding?Pancreatology. 2015 Sep-Oct;15(5):548-553. doi: 10.1016/j.pan.2015.07.002. Epub 2015 Jul 17. Pancreatology. 2015. PMID: 26235830
-
Comparison of different feeding regimes after pancreatoduodenectomy - a retrospective cohort analysis.Nutr J. 2017 Jul 4;16(1):42. doi: 10.1186/s12937-017-0265-2. Nutr J. 2017. PMID: 28676052 Free PMC article.
-
Enteral tube feeding in adults.J R Coll Physicians Edinb. 2015 Mar;45(1):49-54. doi: 10.4997/JRCPE.2015.112. J R Coll Physicians Edinb. 2015. PMID: 25874832 Review.
-
Nasoenteric tube versus jejunostomy for enteral nutrition feeding following major upper gastrointestinal operations: a meta-analysis.Asia Pac J Clin Nutr. 2017 Jan;26(1):20-26. doi: 10.6133/apjcn.112015.05. Asia Pac J Clin Nutr. 2017. PMID: 28049257 Review.
Cited by
-
Current evidence of nutritional therapy in pancreatoduodenectomy: Systematic review of randomized controlled trials.Ann Gastroenterol Surg. 2019 Oct 10;3(6):620-629. doi: 10.1002/ags3.12287. eCollection 2019 Nov. Ann Gastroenterol Surg. 2019. PMID: 31788650 Free PMC article. Review.
-
Enteral nutrition reduces delayed gastric emptying after standard pancreaticoduodenectomy with child reconstruction.J Gastrointest Surg. 2012 May;16(5):1004-11. doi: 10.1007/s11605-012-1821-x. Epub 2012 Jan 19. J Gastrointest Surg. 2012. PMID: 22258876
-
Impact of Obesity on Perioperative Outcomes in Robotic Pancreaticoduodenectomy: A Propensity Score-Matched Study.Int J Med Robot. 2024 Dec;20(6):e70034. doi: 10.1002/rcs.70034. Int J Med Robot. 2024. PMID: 39698987 Free PMC article.
-
Early oral feeding after pancreatoduodenectomy enhances recovery without increasing morbidity.HPB (Oxford). 2014 Jul;16(7):656-64. doi: 10.1111/hpb.12197. Epub 2013 Dec 6. HPB (Oxford). 2014. PMID: 24308458 Free PMC article.
-
Does the Ileal Brake Contribute to Delayed Gastric Emptying After Pancreatoduodenectomy?Dig Dis Sci. 2017 Feb;62(2):319-335. doi: 10.1007/s10620-016-4402-0. Epub 2016 Dec 19. Dig Dis Sci. 2017. PMID: 27995402 Review.
References
-
- Martignoni ME, Friess H, Sell F, et al. Enteral nutrition prolongs delayed gastric emptying in patients after Whipple resection. Am J Surg. 2000;180:18–23. - PubMed
-
- Van Berge Henegouwen MI, van Gulik TM, DeWit LT, et al. Delayed gastric emptying after standard pancreaticoduodenectomy versus pylorus-preserving pancreaticoduodenectomy: an analysis of 200 consecutive patients. J Am Coll Surg. 1997;185:373–379. - PubMed
-
- Horstmann O, Becker H, Post S, et al. Is delayed gastric emptying following pancreaticoduodenectomy related to pylorus preservation? Arch Surg. 1999;384:354–359. - PubMed
-
- Miedema BW, Sarr MG, van Heerden JA, et al. Complications following pancreaticoduodenectomy. Current management. Arch Surg. 1992;127:945–949. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
