

Lymphedema after complete axillary node dissection for melanoma: assessment using a new, objective definition
- PMID: 15492570
- PMCID: PMC1356494
- DOI: 10.1097/01.sla.0000143271.32568.2b
Lymphedema after complete axillary node dissection for melanoma: assessment using a new, objective definition
Abstract
Objectives: The objectives of this study were to define appropriate criteria for assessing the presence of lymphedema, and to report the prevalence and risk factors for development of upper limb lymphedema after level I-III axillary dissection for melanoma.
Summary background data: The lack of a consistent and reliable objective definition for lymphedema remains a significant barrier to appreciating its prevalence after axillary dissection for melanoma (or breast carcinoma).
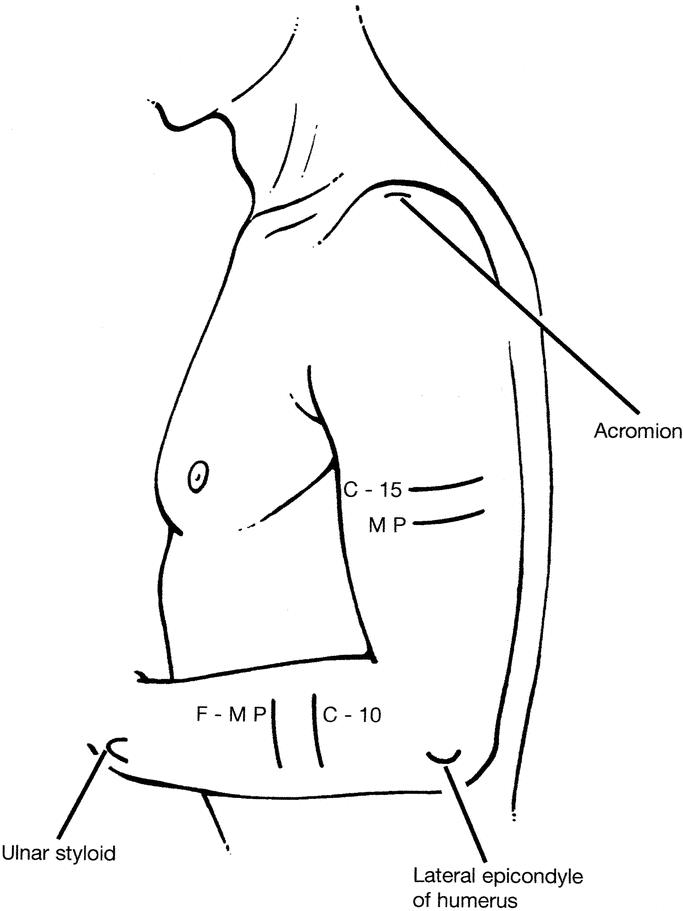
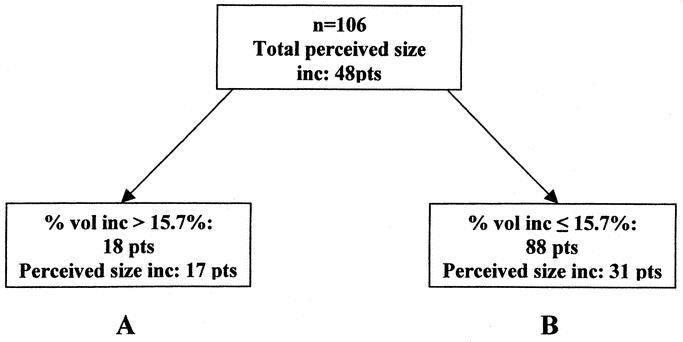
Methods: Lymphedema was assessed in 107 patients (82 male, 25 female) who had previously undergone complete level I-III axillary dissection. Of the 107 patients, 17 had also received postoperative axillary radiotherapy. Arm volume was measured using a water displacement technique. Change in volume of the arm on the side of the dissection was referenced to the volume of the other (control) arm. Volume measurements were corrected for the effect of handedness using corrections derived from a control group. Classification and regression tree (CART) analysis was used to determine a threshold fractional arm volume increase above which volume changes were considered to indicate lymphedema.
Results: Based on the CART analysis results, lymphedema was defined as an increase in arm volume greater than 16% of the volume of the control arm. Using this definition, lymphedema prevalence for patients in the present study was 10% after complete level I-III axillary dissection for melanoma and 53% after additional axillary radiotherapy. Radiotherapy and wound complications were independent risk factors for the development of lymphedema.
Conclusions: A suggested objective definition for arm lymphedema after axillary dissection is an arm volume increase of greater than 16% of the volume of the control arm.
Figures
References
-
- Halsted WS. The swelling of the arm after operations for cancer of the breast—elephantiasis chirurgica—its cause and prevention. Bulletin of the Johns Hopkins Hospital. 1921;32:309–313.
-
- Erickson VS, Pearson ML, Ganz PA, et al. Arm edema in breast cancer patients. J Natl Cancer Inst. 2001;93:96–111. - PubMed
-
- Petrek JA, Heelan MC. Incidence of breast carcinoma-related lymphedema. Cancer. 1998;83:2776–2781. - PubMed
-
- Mansfield PF, Ames FC, Balch CM. Axillary lymph node dissection. In: Balch CM, Houghton AN, Sober AJ, et al., eds. Cutaneous Melanoma, 3rd ed. St. Louis: Quality Medical Publishing; 1998:259–268.
-
- Winer EP, Morrow M, Osbourne CK, et al. Cancer of the breast. In: Devita VT, Hellman S, Rosenberg S, eds. Cancer: Principles and Practice of Oncology, 5th ed. Philadelphia: Lippincott-Raven; 1997:1541–1602.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
