

Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study
- PMID: 15492574
- PMCID: PMC1356498
- DOI: 10.1097/01.sla.0000143301.56154.95
Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study
Abstract
Objective: Determine the histologic response-rate (complete versus partial tumor extinction) after single radiofrequency ablation (RFA) of small hepatocellular carcinoma (HCC) arising in cirrhosis. Investigate possible predictors of response and assess efficacy and safety of RFA as a bridge to liver transplantation (OLT).
Background: RFA has become the elective treatment of local control of HCC, although histologic data supporting radiologic assessment of response are rare and prospective studies are lacking. Prognostic impact of repeated RFA for HCC persistence is also undetermined.
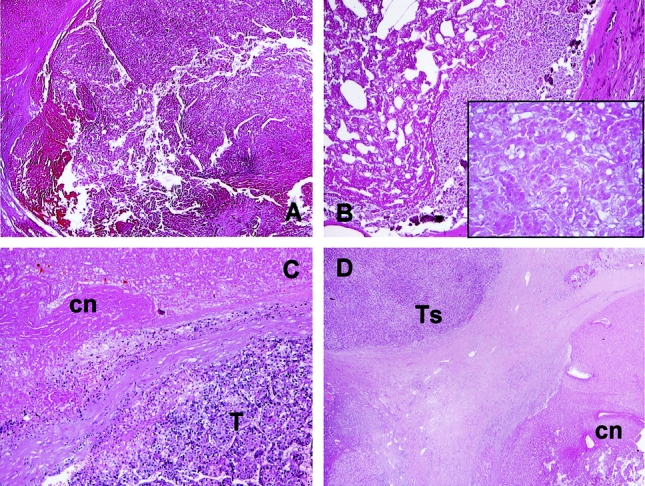
Methods: Percentage of RFA-induced necrosis and tumor persistence-rate at various intervals from treatment was studied in 60 HCC (median: 3 cm; Milan-Criteria IN: 80%) isolated in 50 consecutive cirrhotic patients undergoing OLT. Single-session RFA was the only treatment planned before OLT. Histologic response determined on explanted livers was related to 28 variables and to pre-OLT CT scan.
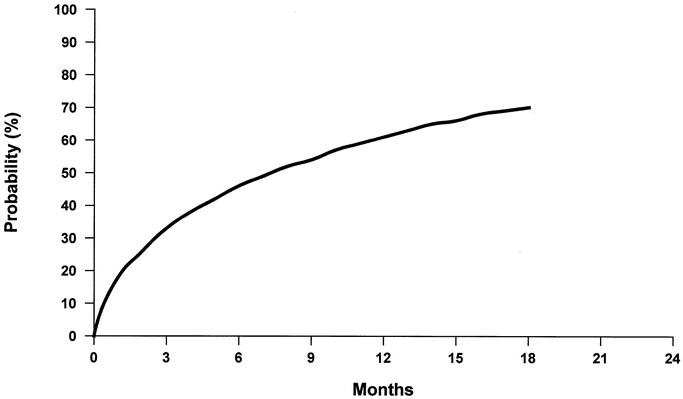
Results: Mean interval RFA-->OLT was 9.5 months. Post-RFA complete response rate was 55%, rising to 63% for HCC </=3 cm. Tumor size was the only prognostic factor significantly related to response (P = 0.007). Tumor satellites and/or new HCC foci (56 nodules) were unaffected by RFA and significantly correlated with HCC >3 cm (P = 0.05). Post-RFA tumor persistence probability increased with time (12 months: 59%; 18 months: 70%). Radiologic response rate was 70%, not significantly different from histology. Major post-RFA morbidity was 8%. No mortality, Child deterioration, patient withdrawal because of tumor progression was observed. Post-OLT 3-year patient/graft survival was 83%.
Conclusions: RFA is a safe and effective treatment of small HCC in cirrhotics awaiting OLT, although tumor size (>3 cm) and time from treatment (>1 year) predict a high risk of tumor persistence in the targeted nodule. RFA should not be considered an independent therapy for HCC.
Figures
References
-
- Mc Gahan JP, Browning PD, Brock JM, et al. Hepatic ablation using radiofrequency electrocautery. Invest Radiol. 1990;25:267–270. - PubMed
-
- Rossi S, Fornari F, Pathies C, et al. Thermal lesions induced by 480KHz localized current field in guinea pig and pig liver. Tumori. 1990;76:54–57. - PubMed
-
- Rossi S, Fornari F, Buscarini L. Percutaneous ultrasound-guided radiofrequency electrocautery for the treatment of small hepatocellular carcinoma. J Interv Radiol. 1993;8:97–103.
-
- Curley SA, Izzo F. Laparoscopic radiofrequency [editorial]. Ann Surg Oncol. 2000;7:78–79. - PubMed
-
- Montorsi M, Santambrogio R, Bianchi P, et al. Radiofrequency interstitial thermal ablation of hepatocellular carcinoma in liver cirrhosis: role of the laparoscopic approach. Surg Endosc. 2001;15:141–145. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
