

Repetitive bilateral arm training and motor cortex activation in chronic stroke: a randomized controlled trial
- PMID: 15494583
- PMCID: PMC2930817
- DOI: 10.1001/jama.292.15.1853
Repetitive bilateral arm training and motor cortex activation in chronic stroke: a randomized controlled trial
Erratum in
- JAMA. 2004 Nov 24;292(20):2470
Abstract
Context: Reorganization in central motor networks occurs during early recovery from hemiparetic stroke. In chronic stroke survivors, specific rehabilitation therapy can improve upper extremity function.
Objective: To test the hypothesis that in patients who have chronic motor impairment following stroke, specific rehabilitation therapy that improves arm function is associated with reorganization of cortical networks.
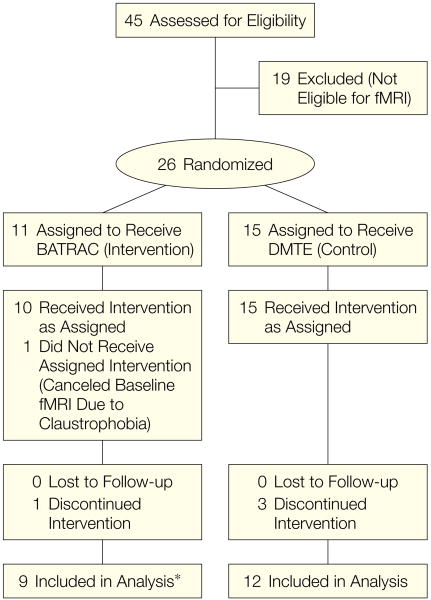
Design, setting, and patients: A randomized controlled clinical trial conducted in a US ambulatory rehabilitation program with 21 patients (median [IQR], 50.3 [34.8-77.3] months after unilateral stroke). Data were collected between 2001 and 2004.
Interventions: Patients were randomly assigned to bilateral arm training with rhythmic auditory cueing (BATRAC) (n = 9) or standardized dose-matched therapeutic exercises (DMTE) (n = 12). Both were conducted for 1 hour, 3 times a week, for 6 weeks.
Main outcome measures: Within 2 weeks before and after the intervention, brain activation during elbow movement assessed by functional magnetic resonance imaging (fMRI) and functional outcome assessed using arm function scores.
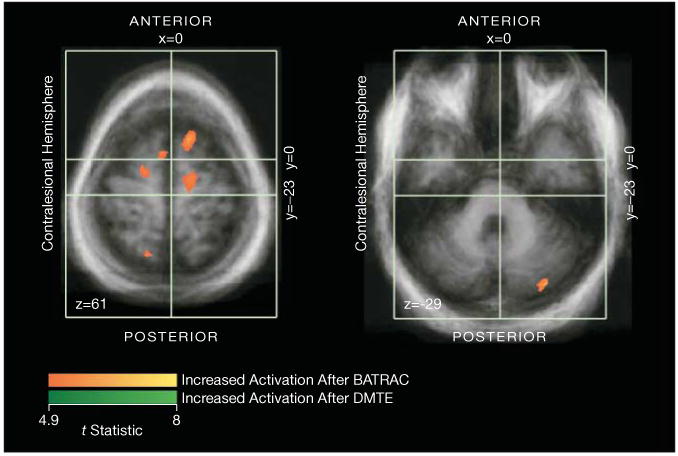
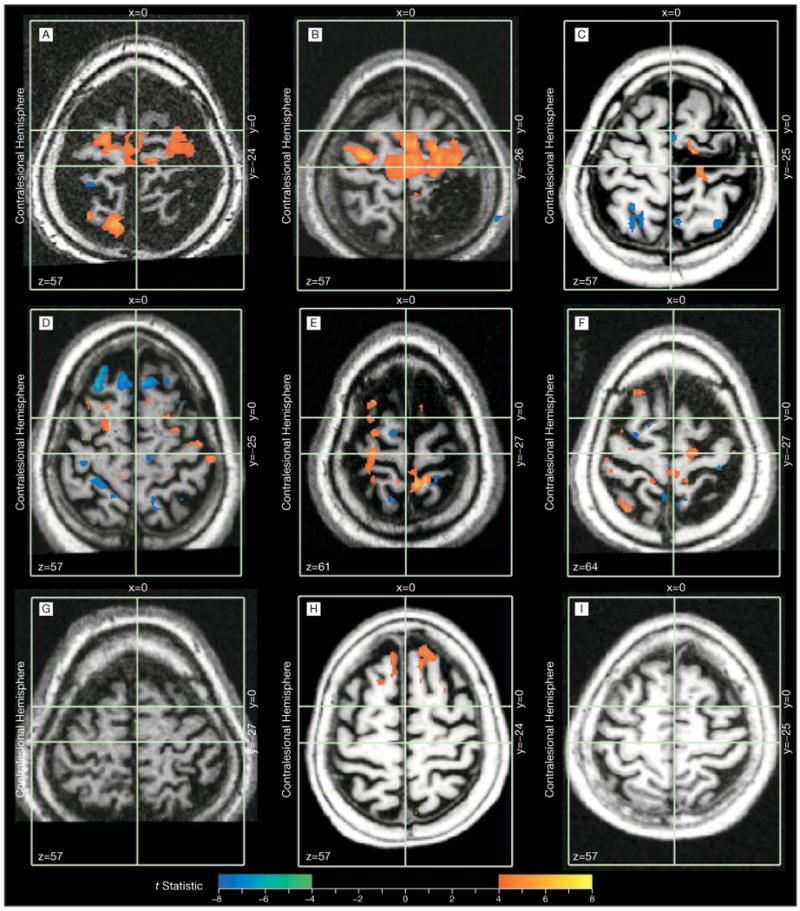
Results: Patients in the BATRAC group but not in the DMTE group increased hemispheric activation during paretic arm movement (P = .03). Changes in activation were observed in the contralesional cerebrum and ipsilesional cerebellum (P = .009). BATRAC was associated with significant increases in activation in precentral (P<.001) and postcentral gyri (P = .03) and the cerebellum (P<.001), although 3 BATRAC patients showed no fMRI changes. Considering all patients, there were no differences in functional outcome between groups. When only BATRAC patients with fMRI response were included (n = 6), BATRAC improved arm function more than DMTE did (P = .02).
Conclusions: These preliminary findings suggest that BATRAC induces reorganization in contralesional motor networks and provide biological plausibility for repetitive bilateral training as a potential therapy for upper extremity rehabilitation in hemiparetic stroke.
Figures
Similar articles
-
Bilateral and unilateral arm training improve motor function through differing neuroplastic mechanisms: a single-blinded randomized controlled trial.Neurorehabil Neural Repair. 2011 Feb;25(2):118-29. doi: 10.1177/1545968310380685. Epub 2010 Oct 7. Neurorehabil Neural Repair. 2011. PMID: 20930212 Free PMC article. Clinical Trial.
-
Temporal and spatial control following bilateral versus unilateral training.Hum Mov Sci. 2008 Oct;27(5):749-58. doi: 10.1016/j.humov.2008.03.006. Epub 2008 Jul 17. Hum Mov Sci. 2008. PMID: 18639360 Clinical Trial.
-
Repetitive bilateral arm training with rhythmic auditory cueing improves motor function in chronic hemiparetic stroke.Stroke. 2000 Oct;31(10):2390-5. doi: 10.1161/01.str.31.10.2390. Stroke. 2000. PMID: 11022069 Clinical Trial.
-
Rehabilitation of arm function after stroke. Literature review.Ann Phys Rehabil Med. 2009 Apr;52(3):269-93. doi: 10.1016/j.rehab.2008.10.003. Epub 2009 Apr 9. Ann Phys Rehabil Med. 2009. PMID: 19398398 Review. English, French.
-
Activation likelihood estimation meta-analysis of motor-related neural activity after stroke.Neuroimage. 2012 Feb 1;59(3):2771-82. doi: 10.1016/j.neuroimage.2011.10.023. Epub 2011 Oct 17. Neuroimage. 2012. PMID: 22023742 Review.
Cited by
-
Biomarkers and predictors of restorative therapy effects after stroke.Curr Neurol Neurosci Rep. 2013 Feb;13(2):329. doi: 10.1007/s11910-012-0329-9. Curr Neurol Neurosci Rep. 2013. PMID: 23299824 Free PMC article. Review.
-
Post-stroke protection from maladaptive effects of learning with the non-paretic forelimb by bimanual home cage experience in C57BL/6 mice.Behav Brain Res. 2013 Sep 1;252:180-7. doi: 10.1016/j.bbr.2013.05.062. Epub 2013 Jun 10. Behav Brain Res. 2013. PMID: 23756140 Free PMC article.
-
Augmented efficacy of intermittent theta burst stimulation on the virtual reality-based cycling training for upper limb function in patients with stroke: a double-blinded, randomized controlled trial.J Neuroeng Rehabil. 2021 May 31;18(1):91. doi: 10.1186/s12984-021-00885-5. J Neuroeng Rehabil. 2021. PMID: 34059090 Free PMC article. Clinical Trial.
-
Mental practice with motor imagery: evidence for motor recovery and cortical reorganization after stroke.Arch Phys Med Rehabil. 2006 Dec;87(12 Suppl 2):S2-11. doi: 10.1016/j.apmr.2006.08.326. Arch Phys Med Rehabil. 2006. PMID: 17140874 Free PMC article. Clinical Trial.
-
ARMin: a robot for patient-cooperative arm therapy.Med Biol Eng Comput. 2007 Sep;45(9):887-900. doi: 10.1007/s11517-007-0226-6. Epub 2007 Aug 3. Med Biol Eng Comput. 2007. PMID: 17674069
References
-
- Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Neurologic and functional recovery: the Copenhagen Stroke Study. Phys Med Rehabil Clin North Am. 1999;10:887–906. - PubMed
-
- Calautti C, Baron JC. Functional neuroimaging studies of motor recovery after stroke in adults: a review. Stroke. 2003;34:1553–1566. - PubMed
-
- Cramer SC, Bastings EP. Mapping clinically relevant plasticity after stroke. Neuropharmacology. 2000;39:842–851. - PubMed
-
- Chollet F, DiPiero V, Wise RJ, Brooks DJ, Dolan RJ, Frackowiak RS. The functional anatomy of motor recovery after stroke in humans: a study with positron emission tomography. Ann Neurol. 1991;29:63–71. - PubMed
-
- Cramer SC, Nelles G, Benson RR, et al. A functional MRI study of subjects recovered from hemiparetic stroke. Stroke. 1997;28:2518–2527. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
