

Modeling the development of acquired clinical immunity to Plasmodium falciparum malaria
- PMID: 15501785
- PMCID: PMC523055
- DOI: 10.1128/IAI.72.11.6538-6545.2004
Modeling the development of acquired clinical immunity to Plasmodium falciparum malaria
Abstract
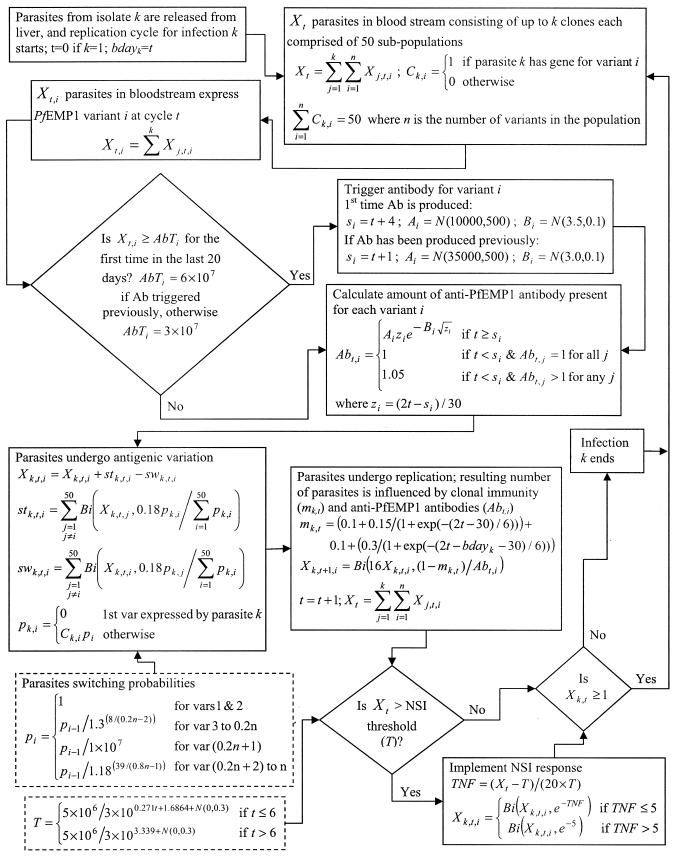
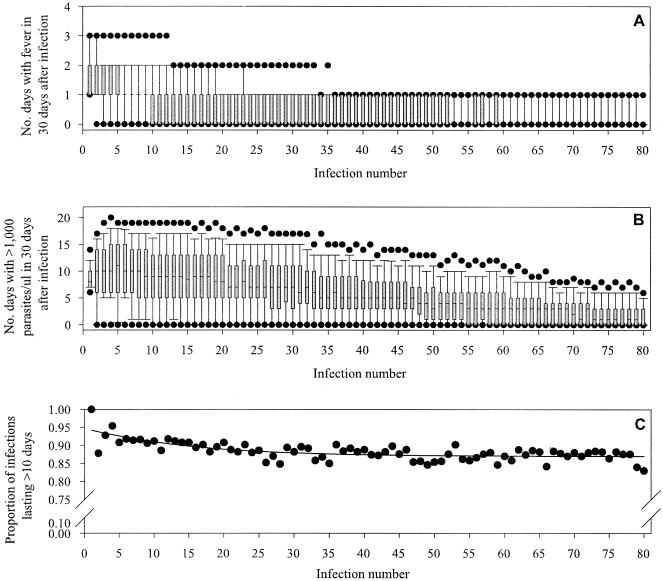
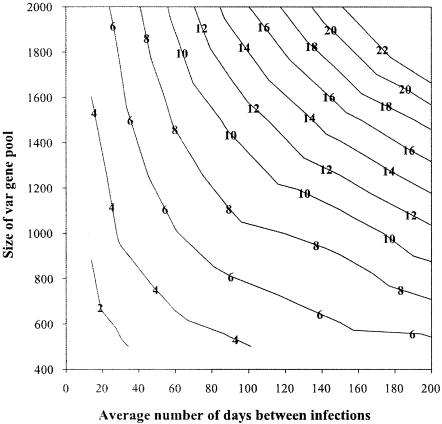
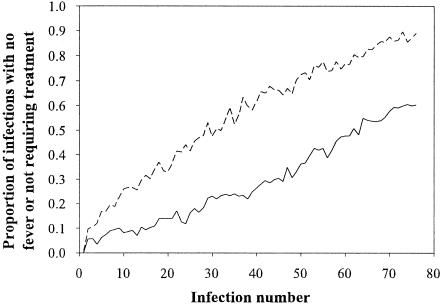
Individuals living in regions where malaria is endemic develop an acquired immunity to malaria which enables them to remain asymptomatic while still carrying parasites. Field studies indicate that cumulative exposure to a variety of diverse Plasmodium parasites is required for the transition from symptomatic to asymptomatic malaria. This study used a simulation model of the within-host dynamics of P. falciparum to investigate the development of acquired clinical immunity under different transmission conditions and levels of parasite diversity. Antibodies developed to P. falciparum erythrocyte membrane protein 1 (PfEMP1), a clonally variant molecule, were assumed to be a key human immunological response to P. falciparum infection, along with responses to clonally conserved but polymorphic antigens. The time to the development of clinical immunity was found to be proportional to parasite diversity and inversely proportional to transmission intensity. The effect of early termination of symptomatic infections by chemotherapy was investigated and found not to inhibit the host's ability to develop acquired immunity. However, the time required to achieve this state was approximately double that compared to when no treatment was administered. This study demonstrates that an immune response primarily targeted against PfEMP1 has the ability to reduce clinical symptoms of infections irrespective of whether treatment is administered, supporting its role in the development of acquired clinical immunity. The results also illustrate a novel use for simulation models of P. falciparum infections, investigation of the influence of intervention strategies on the development of naturally acquired clinical immunity.
Figures
Similar articles
-
Controlled human malaria infection with Plasmodium falciparum demonstrates impact of naturally acquired immunity on virulence gene expression.PLoS Pathog. 2019 Jul 11;15(7):e1007906. doi: 10.1371/journal.ppat.1007906. eCollection 2019 Jul. PLoS Pathog. 2019. PMID: 31295334 Free PMC article. Clinical Trial.
-
Sequential, ordered acquisition of antibodies to Plasmodium falciparum erythrocyte membrane protein 1 domains.J Immunol. 2009 Sep 1;183(5):3356-63. doi: 10.4049/jimmunol.0901331. Epub 2009 Aug 12. J Immunol. 2009. PMID: 19675168
-
IgG antibodies to endothelial protein C receptor-binding cysteine-rich interdomain region domains of Plasmodium falciparum erythrocyte membrane protein 1 are acquired early in life in individuals exposed to malaria.Infect Immun. 2015 Aug;83(8):3096-103. doi: 10.1128/IAI.00271-15. Epub 2015 May 26. Infect Immun. 2015. PMID: 26015475 Free PMC article.
-
Clinical and parasitological studies on immunity to Plasmodium falciparum malaria in children.Scand J Infect Dis Suppl. 1996;102:1-53. Scand J Infect Dis Suppl. 1996. PMID: 9060051 Review.
-
PfEMP1 - A Parasite Protein Family of Key Importance in Plasmodium falciparum Malaria Immunity and Pathogenesis.Adv Parasitol. 2015 Apr;88:51-84. doi: 10.1016/bs.apar.2015.02.004. Epub 2015 Mar 23. Adv Parasitol. 2015. PMID: 25911365 Review.
Cited by
-
A metapopulation model for malaria with transmission-blocking partial immunity in hosts.J Math Biol. 2012 Feb;64(3):423-48. doi: 10.1007/s00285-011-0418-4. Epub 2011 Mar 26. J Math Biol. 2012. PMID: 21442182
-
Determination of the processes driving the acquisition of immunity to malaria using a mathematical transmission model.PLoS Comput Biol. 2007 Dec;3(12):e255. doi: 10.1371/journal.pcbi.0030255. Epub 2007 Nov 14. PLoS Comput Biol. 2007. PMID: 18166074 Free PMC article.
-
On the coupling of two models of the human immune response to an antigen.Biomed Res Int. 2014;2014:410457. doi: 10.1155/2014/410457. Epub 2014 Jul 22. Biomed Res Int. 2014. PMID: 25140313 Free PMC article.
-
Modeling the Impact of Bed-Net Use and Treatment on Malaria Transmission Dynamics.Int Sch Res Notices. 2017 Aug 1;2017:6182492. doi: 10.1155/2017/6182492. eCollection 2017. Int Sch Res Notices. 2017. PMID: 28835913 Free PMC article.
-
Mathematical modeling of malaria infection with innate and adaptive immunity in individuals and agent-based communities.PLoS One. 2012;7(3):e34040. doi: 10.1371/journal.pone.0034040. Epub 2012 Mar 28. PLoS One. 2012. PMID: 22470511 Free PMC article.
References
-
- Askjaer, N., C. Maxwell, W. Chambo, T. Staalsoe, M. Nielsen, L. Hviid, C. Curtis, and T. G. Theander. 2001. Insecticide-treated bed nets reduce plasma antibody levels and limit the repertoire of antibodies to Plasmodium falciparum variant surface antigens. Clin. Diagn. Lab. Immunol. 8:1289-1291. - PMC - PubMed
-
- Babiker, H. A., L. C. Ranford-Cartwright, D. Currie, J. D. Charlwood, P. Billingsley, T. Teuscher, and D. Walliker. 1994. Random mating in a natural population of the malaria parasite Plasmodium falciparum. Parasitology 109:413-421. - PubMed
-
- Baird, J. K., M. J. Barcus, R. F. Elyazar, M. J. Bangs, J. D. Maguire, D. J. Fryauff, T. L. Richie, Sekartuti, and W. Kalalo. 2003. Onset of clinical immunity to Plasmodium falciparum among Javanese migrants to Indonesian Papua. Ann. Trop. Med. Parasitol. 97:557-564. - PubMed
-
- Baird, J. K., T. R. Jones, E. W. Danudirgo, B. A. Annis, M. J. Bangs, H. Basri, Purnomo, and S. Masbar. 1991. Age-dependent acquired protection against Plasmodium falciparum in people having two years exposure to hyperendemic malaria. Am. J. Trop. Med. Hyg. 45:65-76. - PubMed
-
- Belizario, V. Y., A. Saul, M. D. Bustos, M. A. Lansang, C. J. Pasay, M. Gatton, and N. P. Salazar. 1997. Field epidemiological studies on malaria in a low endemic area in the Philippines. Acta Trop. 63:241-256. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
