

Intratumoral injection of cyanoacrylate glue in head and neck paragangliomas
- PMID: 15502121
- PMCID: PMC7976413
Intratumoral injection of cyanoacrylate glue in head and neck paragangliomas
Abstract
Background and purpose: Substantial intraoperative bleeding during surgical removal of head and neck paragangliomas may be a major problem in the management of these highly vascularized tumors. Traditional preoperative embolization via a transarterial approach has proved beneficial but is often limited by complex vascular anatomy and unfavorable locations. We report our experience with the preoperative devascularization of head and neck paragangliomas by using direct puncture and an intralesional injection of cyanoacrylate.
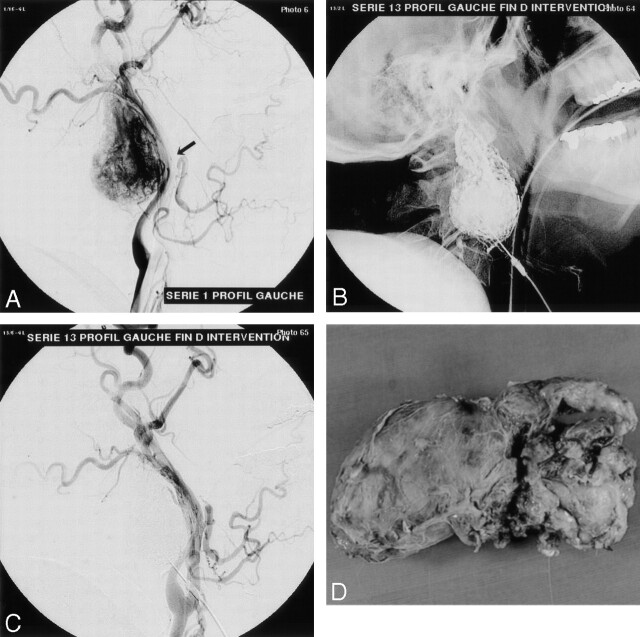
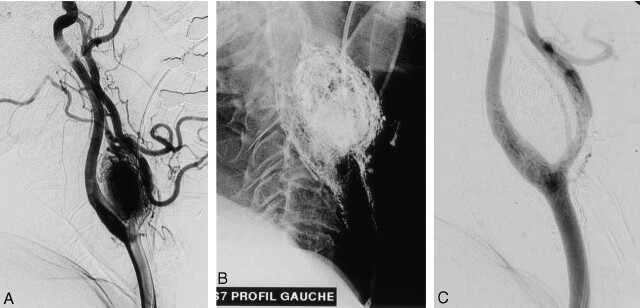
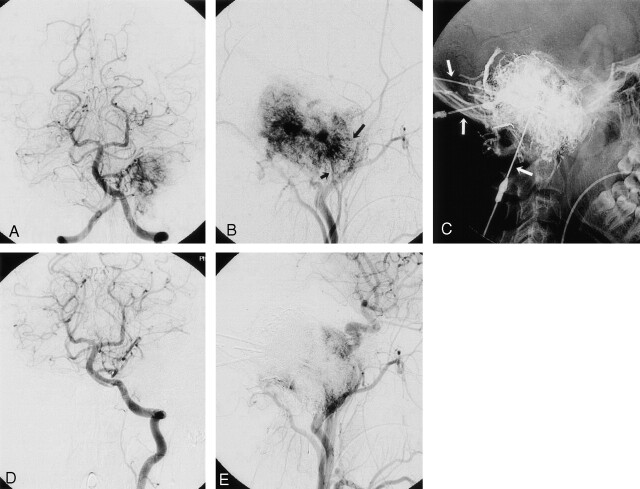
Methods: We retrospectively analyzed nine consecutive patients with head and neck paragangliomas who were referred for preoperative devascularization. Three patients were treated for carotid-body tumors; two for vagal lesions; and four, for jugular paragangliomas. Direct puncture of the lesion was performed by using roadmap fluoroscopic guidance. Acrylic glue was injected by using continuous biplane fluoroscopy. All patients underwent postembolization control angiography and immediate postoperative CT scanning.
Results: Angiograms showed that complete devascularization was achieved in all cervical glomus tumors, whereas subtotal devascularization was achieved in jugular paragangliomas. In this latter location, the injection of acrylic glue was limited by the potential risk of reflux into normal brain territory via feeders from the internal carotid or vertebral artery. The tumors were surgically removed and histologically examined. No technical or clinical complications related to the embolization procedure occurred.
Conclusion: Percutaneous puncture of paragangliomas in the head and neck region and their preoperative devascularization by intralesional injection of acrylic glue is a feasible, safe, and effective technique.
Copyright American Society of Neuroradiology
Figures
Comment in
-
Direct puncture embolization for paragangliomas: promising results but preliminary data.AJNR Am J Neuroradiol. 2004 Oct;25(9):1453-4. AJNR Am J Neuroradiol. 2004. PMID: 15502118 Free PMC article. No abstract available.
References
-
- Erickson D, Kudva YC, Ebersold MJ, et al. Benign paragangliomas: clinical presentation and treatment outcomes in 236 patients. J Clin Endocrinol Metab 2001;86:5210–5216 - PubMed
-
- Bishop GB Jr, Urist MM, el Gammal T, et al. Paragangliomas of the neck. Arch Surg 1992;127:1441–1445 - PubMed
-
- Somasundar P, Krouse R, Hostetter R, et al. Paragangliomas: a decade of clinical experience. J Surg Oncol 2000;74:286–290 - PubMed
-
- Patetsios P, Gable DR, Garrett WV, et al. Management of carotid body paragangliomas and review of a 30-year experience. Ann Vasc Surg 2002;16:331–338 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical