

Multimodal pressure-flow method to assess dynamics of cerebral autoregulation in stroke and hypertension
- PMID: 15504235
- PMCID: PMC529459
- DOI: 10.1186/1475-925X-3-39
Multimodal pressure-flow method to assess dynamics of cerebral autoregulation in stroke and hypertension
Abstract
Background: This study evaluated the effects of stroke on regulation of cerebral blood flow in response to fluctuations in systemic blood pressure (BP). The autoregulatory dynamics are difficult to assess because of the nonstationarity and nonlinearity of the component signals.
Methods: We studied 15 normotensive, 20 hypertensive and 15 minor stroke subjects (48.0 +/- 1.3 years). BP and blood flow velocities (BFV) from middle cerebral arteries (MCA) were measured during the Valsalva maneuver (VM) using transcranial Doppler ultrasound.
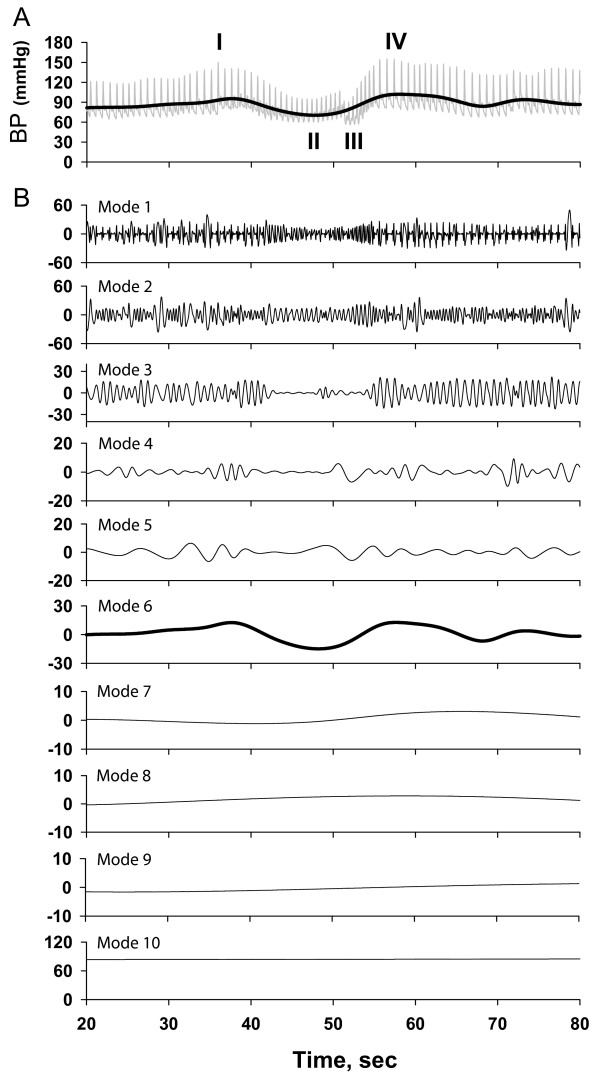
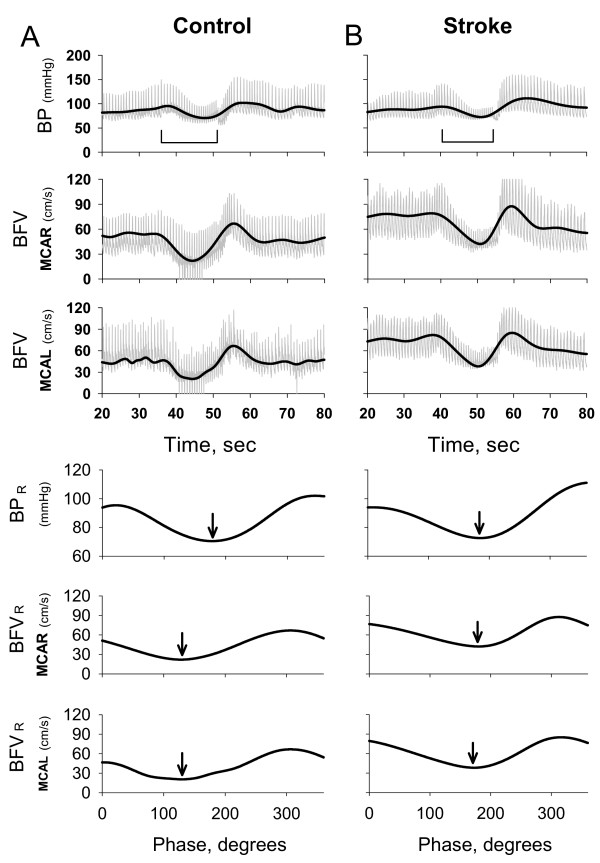
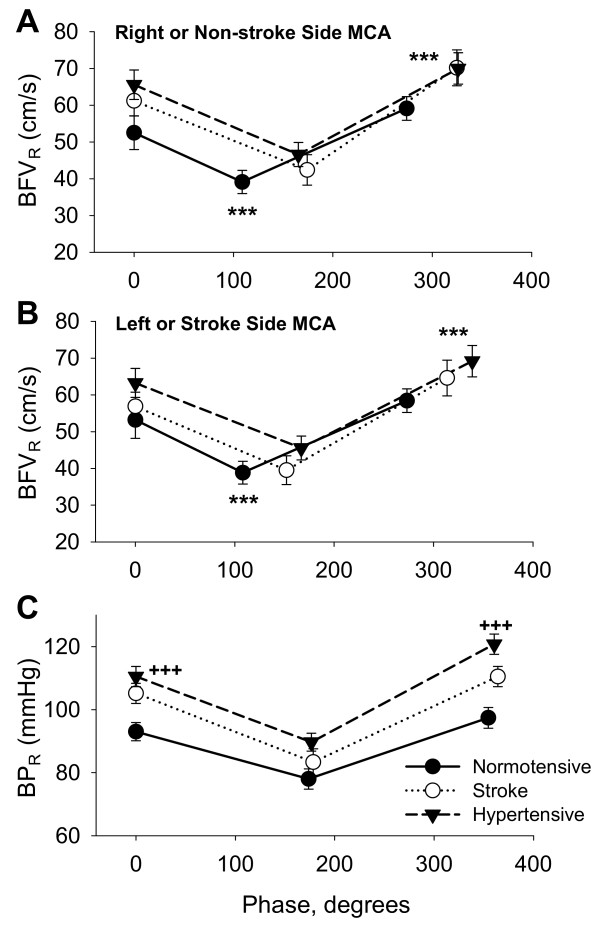
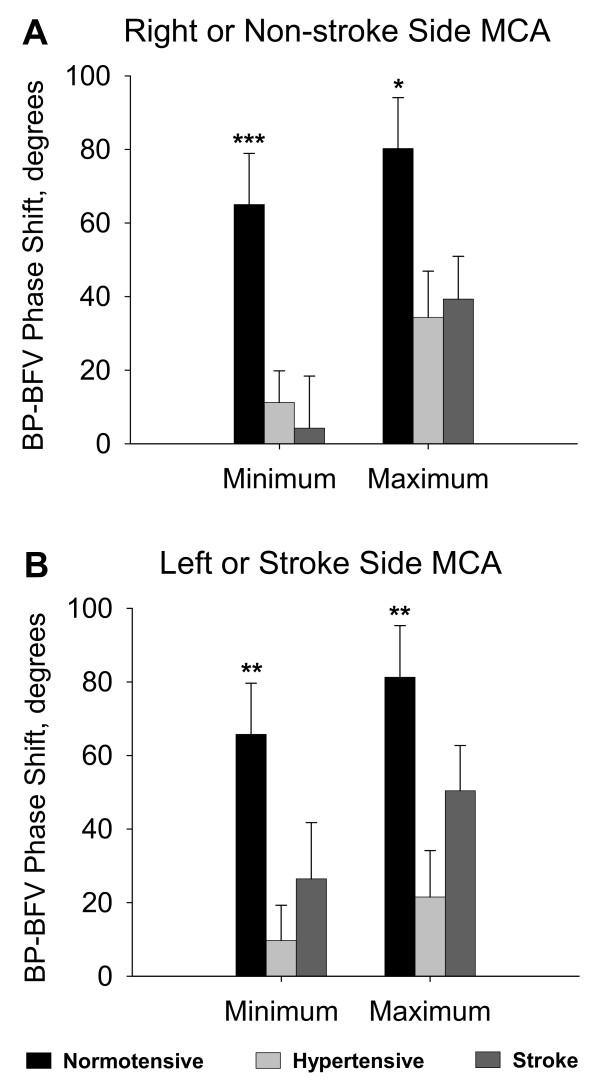
Results: A new technique, multimodal pressure-flow analysis (MMPF), was implemented to analyze these short, nonstationary signals. MMPF analysis decomposes complex BP and BFV signals into multiple empirical modes, representing their instantaneous frequency-amplitude modulation. The empirical mode corresponding to the VM BP profile was used to construct the continuous phase diagram and to identify the minimum and maximum values from the residual BP (BPR) and BFV (BFVR) signals. The BP-BFV phase shift was calculated as the difference between the phase corresponding to the BPR and BFVR minimum (maximum) values. BP-BFV phase shifts were significantly different between groups. In the normotensive group, the BFVR minimum and maximum preceded the BPR minimum and maximum, respectively, leading to large positive values of BP-BFV shifts.
Conclusion: In the stroke and hypertensive groups, the resulting BP-BFV phase shift was significantly smaller compared to the normotensive group. A standard autoregulation index did not differentiate the groups. The MMPF method enables evaluation of autoregulatory dynamics based on instantaneous BP-BFV phase analysis. Regulation of BP-BFV dynamics is altered with hypertension and after stroke, rendering blood flow dependent on blood pressure.
Figures
References
-
- Zhang R, Zuckerman JH, Giller CA, Levine BD. Transfer function analysis of dynamic cerebral autoregulation in humans. Am J Physiol. 1998;274:H233–41. - PubMed
-
- Tiecks FP, Lam AM, Matta BF, Strebel S, Douville C, Newell DW. Effects of the Valsalva maneuver on cerebral circulation in healthy adults. A transcranial Doppler Study. Stroke. 1995;26:1386–1392. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
