

Computational cardiac anatomy using MRI
- PMID: 15508155
- PMCID: PMC1317108
- DOI: 10.1002/mrm.20255
Computational cardiac anatomy using MRI
Abstract
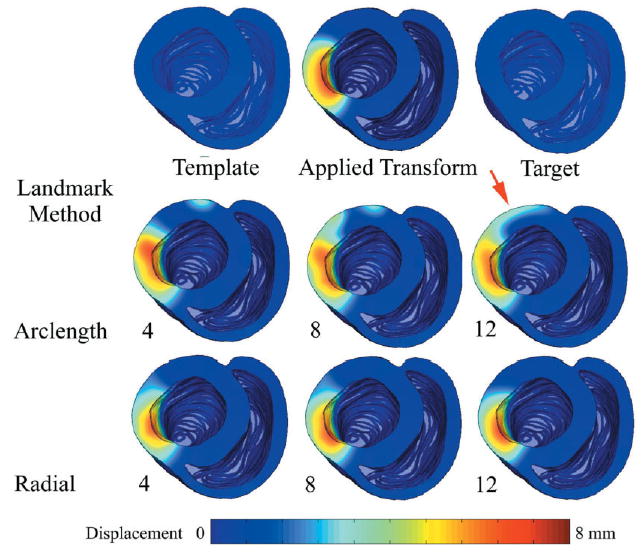
Ventricular geometry and fiber orientation may undergo global or local remodeling in cardiac disease. However, there are as yet no mathematical and computational methods for quantifying variation of geometry and fiber orientation or the nature of their remodeling in disease. Toward this goal, a landmark and image intensity-based large deformation diffeomorphic metric mapping (LDDMM) method to transform heart geometry into common coordinates for quantification of shape and form was developed. Two automated landmark placement methods for modeling tissue deformations expected in different cardiac pathologies are presented. The transformations, computed using the combined use of landmarks and image intensities, yields high-registration accuracy of heart anatomies even in the presence of significant variation of cardiac shape and form. Once heart anatomies have been registered, properties of tissue geometry and cardiac fiber orientation in corresponding regions of different hearts may be quantified.
(c) 2004 Wiley-Liss, Inc.
Figures





References
-
- Prinzen FW, Cheriex EC, Delhaas T, van Oosterhout MF, Arts T, Wellens HJ, Reneman RS. Asymmetric thickness of the left ventricular wall resulting from asynchronous electric activation: a study in dogs with ventricular pacing and in patients with left bundle branch block. Am Heart J. 1995;130:1045–1053. - PubMed
-
- van Oosterhout MF, Prinzen FW, Arts T, Schreuder JJ, Vanagt WY, Cleutjens JP, Reneman RS. Asynchronous electrical activation induces asymmetrical hypertrophy of the left ventricular wall. Circulation. 1998;98:588–595. - PubMed
-
- van Oosterhout MF, Arts T, Muijtjens AM, Reneman RS, Prinzen FW. Remodeling by ventricular pacing in hypertrophying dog hearts. Cardiovasc Res. 2001;49:771–778. - PubMed
-
- van Oosterhout MF, Arts T, Bassingthwaighte JB, Reneman RS, Prinzen FW. Relation between local myocardial growth and blood flow during chronic ventricular pacing. Cardiovasc Res. 2002;53:831–840. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
