

My approach to atypical melanocytic lesions
- PMID: 15509670
- PMCID: PMC1770470
- DOI: 10.1136/jcp.2003.008516
My approach to atypical melanocytic lesions
Abstract
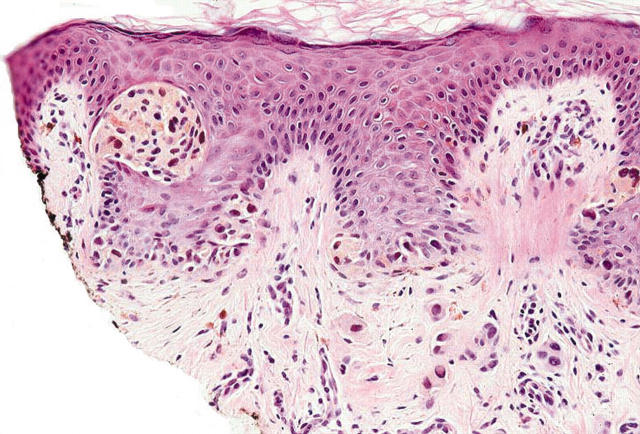
Histological assessment of melanocytic naevi constitutes a substantial proportion of a dermatopathologist's daily workload. Although they may be excised for cosmetic reasons, most lesions encountered are clinically atypical and are biopsied or excised to exclude melanoma. Although dysplastic naevi are most often encountered, cytological atypia may be a feature of several other melanocytic lesions, including genital type naevi, acral naevi, recurrent naevi, and neonatal or childhood naevi. With greater emphasis being given to cosmetic results, and because of an ever increasing workload, several "quicker and less traumatising" techniques have been introduced in the treatment and diagnosis of atypical naevi including punch, shave, and scoop shave biopsies. A major limitation to all of these alternatives is that often only part of the lesion is available for histological assessment and therefore all too frequently the pathologist's report includes a recommendation for complete excision so that the residual lesion can be studied. Complete or large excision of all clinically atypical naevi permits histological assessment of the entire lesion, and in most cases spares the patient the need for further surgical intervention.
Figures
Similar articles
-
Histopathological characteristics of small diameter melanocytic naevi.J Clin Pathol. 2003 Jun;56(6):459-64. doi: 10.1136/jcp.56.6.459. J Clin Pathol. 2003. PMID: 12783974 Free PMC article.
-
The usefulness of single and combined clinical characteristics for the diagnosis of dysplastic naevi.Melanoma Res. 1992 Jan-Feb;1(5-6):377-83. doi: 10.1097/00008390-199201000-00009. Melanoma Res. 1992. PMID: 1422193
-
The ultrastructure of dysplastic naevi: comparison with superficial spreading melanoma and common naevocellular naevi.Arch Dermatol Res. 1990;282(6):353-62. doi: 10.1007/BF00372084. Arch Dermatol Res. 1990. PMID: 2260880
-
[Dysplastic melanocytic nevus].Duodecim. 2010;126(21):2492-501. Duodecim. 2010. PMID: 21171474 Review. Finnish.
-
The approach to the patient with a difficult melanocytic lesion.Pathology. 2004 Oct;36(5):428-34. doi: 10.1080/00313020412331283905. Pathology. 2004. PMID: 15370112 Review.
Cited by
-
Recurrence of Dysplastic Nevi Is Strongly Associated with Extension of the Lesions to the Lateral Margins and into the Deep Margins through the Hair Follicles in the Original Shave Removal Specimens.Dermatol Res Pract. 2016;2016:8523947. doi: 10.1155/2016/8523947. Epub 2016 Sep 28. Dermatol Res Pract. 2016. PMID: 27774100 Free PMC article.
-
Low rates of clinical recurrence after biopsy of benign to moderately dysplastic melanocytic nevi.J Am Acad Dermatol. 2010 Apr;62(4):591-6. doi: 10.1016/j.jaad.2009.06.080. Epub 2009 Dec 16. J Am Acad Dermatol. 2010. PMID: 20018406 Free PMC article.
-
[Melanocytic nevi at special anatomical sites].Pathologe. 2007 Nov;28(6):430-6. doi: 10.1007/s00292-007-0941-7. Pathologe. 2007. PMID: 17874107 German.
-
Distinguishing between benign and malignant melanocytic nevi by in vivo multiphoton microscopy.Cancer Res. 2014 May 15;74(10):2688-97. doi: 10.1158/0008-5472.CAN-13-2582. Epub 2014 Mar 31. Cancer Res. 2014. PMID: 24686168 Free PMC article.
-
Image and statistical analysis of melanocytic histology.Histopathology. 2012 Sep;61(3):436-44. doi: 10.1111/j.1365-2559.2012.04229.x. Epub 2012 Jun 11. Histopathology. 2012. PMID: 22687043 Free PMC article.
References
-
- Ball NJ, Golitz LE. Melanocytic nevi with focal atypical epithelioid cell components: a review of seventy-three cases. J Am Acad Dermatol 1994;30:724–9. - PubMed
-
- Zembowicz A , McCusker M, Chiarelli C, et al. Morphological analysis of nevoid melanoma: A study of 20 cases with a review of the literature. Am J Dermatopathol 2001;23:167–75. - PubMed
-
- Suster S , Ronnen M, Bubis JJ. Verrucous pseudonevoid melanoma. J Surg Oncol 1987;36:134–37. - PubMed
-
- Wong TY, Suster S, Duncan LM, et al. Nevoid melanoma: a clinicopathological study of seven cases of malignant melanoma mimicking spindle and epithelioid cell nevus and verrucous dermal nevus. Hum Pathol 1995;26:171–9. - PubMed
-
- Li LL, Crotty KA, McCarthy SW, et al. A zonal comparison of MIB1-Ki67 immunoreactivity in benign and malignant melanocytic lesions. Am J Dermatopathol 2000;22:489–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical