

Transabdominal ultrasonography in preoperative staging of gastric cancer
- PMID: 15526355
- PMCID: PMC4576217
- DOI: 10.3748/wjg.v10.i23.3399
Transabdominal ultrasonography in preoperative staging of gastric cancer
Abstract
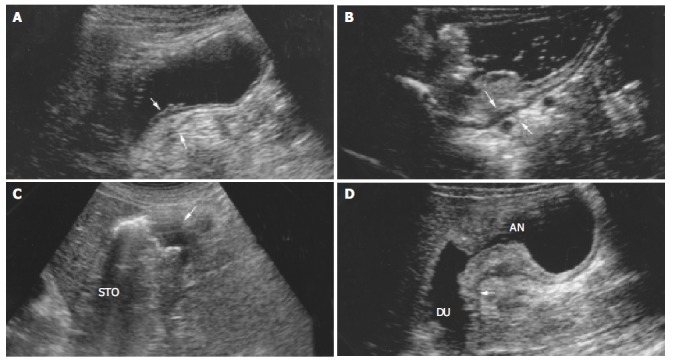
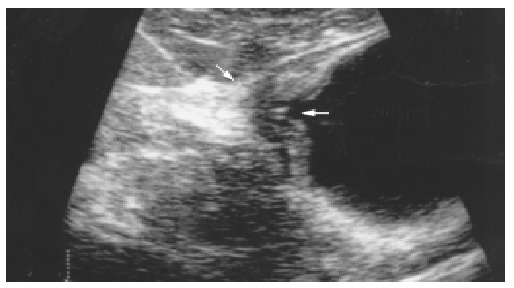
Aim: To investigate the value of transabdominal ultrasonography (US) in the preoperative staging of gastric cancer.
Methods: A total of 198 patients with gastric cancer underwent preoperatively transabdominal US, depth of tumor infiltration was assessed in 125 patients, and lymph node metastasis was assessed in 106 patients.
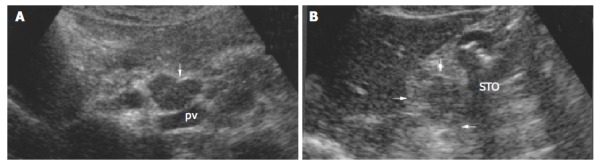
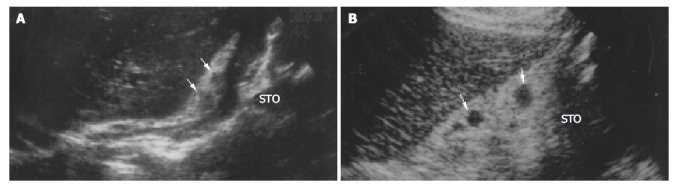
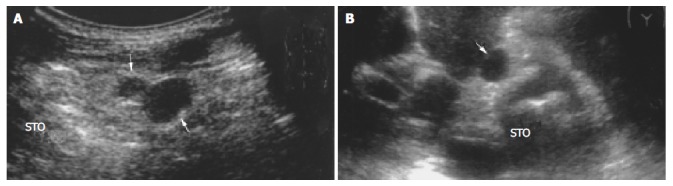
Results: The staging accuracy of transabdominal US was 55.6%, 75.0%, 87.3% and 71.1% in T1, T2, T3 and T4 carcinomas, respectively. The overall accuracy was 77.6%. The detection rate for pancreatic invasion and liver invasion was 77.4%, 71.4%, respectively. The sensitivity, specificity, accuracy of transabdominal US in assessment of lymph node metastasis were 77.6%, 64.1%, 72.6%, respectively. Various shapes such as round, ovoid, spindle were encountered in benign and malignant lymph nodes. Majority of both benign and malignant lymph nodes were hyperechoic and had a distinct border. Benign lymph nodes were smaller than malignant lymph nodes in length and width (P = 0.000, 0.005). Irregular shape, fusional shape, infiltrative signs, inhomogenous echo were seen mainly in malignant lymph nodes (P = 0.045, 0.006, 0.027, 0.006).
Conclusion: Transabdominal US is useful for preoperative staging in gastric cancer, although it is difficult to differentiate benign from malignant lymph nodes.
Figures
Similar articles
-
Usefulness of endoscopic ultrasonography in preoperative TNM staging of gastric cancer.World J Gastroenterol. 2006 Jan 7;12(1):43-7. doi: 10.3748/wjg.v12.i1.43. World J Gastroenterol. 2006. PMID: 16440415 Free PMC article.
-
[Diagnostic value of double contrast-enhanced ultrasonography in preoperative staging of gastric cancer].Zhonghua Zhong Liu Za Zhi. 2009 Sep;31(9):701-4. Zhonghua Zhong Liu Za Zhi. 2009. PMID: 20021869 Chinese.
-
[Application of endoscopic ultrasonography to preoperative clinical staging of esophageal cancer].Ai Zheng. 2005 Nov;24(11):1358-62. Ai Zheng. 2005. PMID: 16552963 Chinese.
-
State-of-the-art preoperative staging of gastric cancer by MDCT and magnetic resonance imaging.World J Gastroenterol. 2014 Apr 28;20(16):4546-57. doi: 10.3748/wjg.v20.i16.4546. World J Gastroenterol. 2014. PMID: 24782607 Free PMC article. Review.
-
Preoperative workflow for lymph nodes staging.Int J Comput Assist Radiol Surg. 2009 Jan;4(1):99-104. doi: 10.1007/s11548-008-0272-z. Epub 2008 Oct 28. Int J Comput Assist Radiol Surg. 2009. PMID: 20033607 Review.
Cited by
-
Clinical Study on the Evaluation of the Condition of Patients with Gastric Tumors and the Choice of Surgical Treatment by Gastric Ultrasonic Filling Method.Contrast Media Mol Imaging. 2022 Jun 9;2022:3960929. doi: 10.1155/2022/3960929. eCollection 2022. Contrast Media Mol Imaging. 2022. PMID: 35800228 Free PMC article.
-
Nomograms Integrating MRI-derived Apparent Diffusion Coefficient and Clinicopathologic Features for Prediction of Axillary Lymph Node Metastasis in Breast Cancer.Radiol Imaging Cancer. 2025 Mar;7(2):e240202. doi: 10.1148/rycan.240202. Radiol Imaging Cancer. 2025. PMID: 40116606 Free PMC article.
-
Risk stratification of gastric cancer screening in community population based on oral contrast-enhanced ultrasonography examination: A 3-year follow-up analysis report.Front Oncol. 2023 Oct 30;13:1218800. doi: 10.3389/fonc.2023.1218800. eCollection 2023. Front Oncol. 2023. PMID: 38023168 Free PMC article.
-
Imaging in assessing lymph node status in gastric cancer.Gastric Cancer. 2009;12(1):6-22. doi: 10.1007/s10120-008-0492-5. Epub 2009 Apr 24. Gastric Cancer. 2009. PMID: 19390927 Review.
-
Validation of the prognostic impact of the new tumor-node-metastasis clinical staging in patients with gastric cancer.Gastric Cancer. 2019 Jan;22(1):123-129. doi: 10.1007/s10120-018-0799-9. Epub 2018 Jan 22. Gastric Cancer. 2019. PMID: 29357013
References
-
- Sipponen P, Järvi O, Kekki M, Siurala M. Decreased incidences of intestinal and diffuse types of gastric carcinoma in Finland during a 20-year period. Scand J Gastroenterol. 1987;22:865–871. - PubMed
-
- Silverberg E. Cancer statistics, 1980. CA Cancer J Clin. 1980;30:23–38. - PubMed
-
- Gelfand DW, Ott DJ. Single- vs. double-contrast gastrointestinal studies: critical analysis of reported statistics. AJR Am J Roentgenol. 1981;137:523–528. - PubMed
-
- White RM, Levine MS, Enterline HT, Laufer I. Early gastric cancer. Recent experience. Radiology. 1985;155:25–27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
