

Surgical treatment and prognosis of gastric cancer in 2,613 patients
- PMID: 15526356
- PMCID: PMC4576218
- DOI: 10.3748/wjg.v10.i23.3405
Surgical treatment and prognosis of gastric cancer in 2,613 patients
Abstract
Aim: To analyze the factors influencing the prognosis of patients with gastric cancer after surgical treatment, in order to optimize the surgical procedures.
Methods: A retrospective study of 2 613 consecutive patients with gastric cancer was performed. Of these patients, 2,301 (88.1%) received operations; 196 explorative laparotomy (EL), 130 by-pass procedure (BPP), and 1 975 surgical resection of the tumors (891 palliative resection and 1 084 curative resection). The survival rate was calculated by the actuarial life table method, and the prognostic factors were evaluated using the Cox regression proportional hazard model.
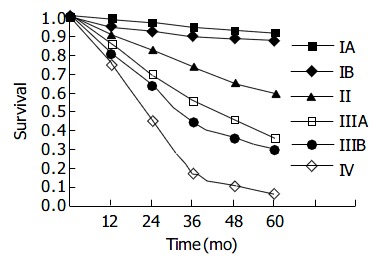
Results: Of the patients, 2,450 (93.8%) were followed-up. The median survival period was 4.6 mo for patients without operation, 5.2 mo for EL, 6.4 mo for BPP, and 15.2 mo for palliative resection (P = 0.0001). Of the patients with surgical resection of the tumors, the overall 1, 3 and 5-year survival rates after were 82.7%, 46.3% and 31.1%, respectively, with the 5-year survival rate being 51.2% in patients with curative resection, and 7.8% for those with palliative resection. The 5-year survival rate was 32.5% for patients with total gastrectomy, and 28.3% for those with total gastrectomy plus resection of the adjacent organs. The factors that independently correlated with poor survival included advanced stage, upper third location, palliative resection, poor differentiation, type IV of Borrmann classification, tumor metastasis (N3), tumor invasion into the serosa and contiguous structure, proximal subtotal gastrectomy for upper third carcinoma and D1 lymphadenectomy after curative treatment.
Conclusion: The primary lesion should be resected as long as the local condition permitted for stage III and IV tumors, in order to prolong the patients' survival and improve their quality of life after operation. Total gastrectomy is indicated for carcinomas in the cardia and fundus, and gastric cancer involving the adjacent organs without distant metastasis requires gastrectomy with resection of the involved organs.
Figures
References
-
- Abeloff MD, Armitage JO, Lichter AS, Niederhuber JE. Clini-cal Oncology. Second edition. China Science Press Harcourt Asia China. 2001:1545–1585.
-
- Price P, Sikore K, Treatment of cancer. 4th edition London. New york NewDeLHI Arnold press. 2002:583–599.
-
- Pisani P, Parkin DM, Bray F, Ferlay J. Erratum: Estimates of the worldwide mortality from 25 cancers in 1990. Int. J. Cancer, 83, 18-29 (1999) Int J Cancer. 1999;83:870–873. - PubMed
-
- World Health Organization, the world health report. Geneva WHO 1997
-
- Sun X, Mu R, Zhou Y, Dai X, Qiao Y, Zhang S, Huangfu X, Sun J, Li L, Lu F. [1990-1992 mortality of stomach cancer in China] Zhonghua Zhongliu Zazhi. 2002;24:4–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
