

Diagnostic relevance of immunoglobulin G avidity for hepatitis A virus
- PMID: 15528704
- PMCID: PMC525178
- DOI: 10.1128/JCM.42.11.5121-5124.2004
Diagnostic relevance of immunoglobulin G avidity for hepatitis A virus
Abstract
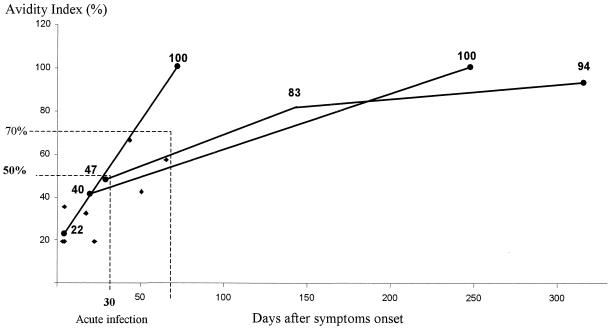
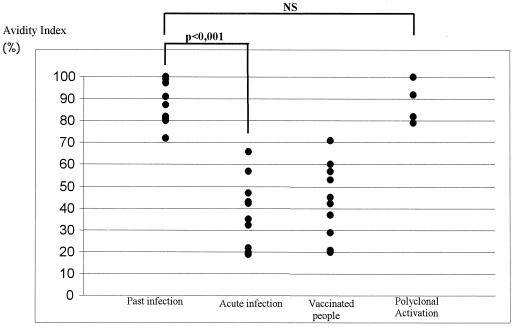
Diagnosis of acute hepatitis A virus (HAV) infection is based on the detection of HAV immunoglobulin M (IgM). However, IgM could be detected due to nonspecific polyclonal activation of the immune system. An avidity test for anti-HAV IgG was developed to distinguish acute infection, where low-avidity antibodies are detected, from immune reactivation. The assay was tested on 104 samples, including 11 sera from patients with past infection, 15 sera from patients with acute infection and 4 collected after recovery, 10 sera from vaccinated subjects, 4 sera from patients with suspected immune reactivation, and 60 unselected HAV-IgM positive sera, collected over 1 year in a routine laboratory. The avidity index (AI) was expressed as percentage. The results were provided as the mean +/- one standard deviation. Patients with a history of prior infection had AIs of >70% (mean, 86% +/- 10), whereas the mean AI was 36% +/- 16 during acute HAV infection (P < 0.001). Within the first month after the onset of hepatitis, avidity was either noncalculable due to a very low IgG titer or <50%. In patients with immune reactivation, avidity was >70% (88% +/- 10%), a finding consistent with a prior infection. Among the 60 unselected sera, 35 (58%) had a noncalculable or <50% avidity, and most of them had a detectable HAV RNA, confirming HAV infection. In contrast, 16 (27%) had an avidity of >70%, and none was reverse transcription-PCR positive, suggesting immune reactivation. These 16 patients were significantly older than the others (50 +/- 16 years versus 26 +/- 14 years). The new anti-HAV IgG avidity assay we developed could improve HAV infection diagnosis, particularly in elderly patients.
Figures
Similar articles
-
Validation of HAV biomarker 2A for differential diagnostic of hepatitis A infected and vaccinated individuals using multiplex serology.Vaccine. 2017 Oct 13;35(43):5883-5889. doi: 10.1016/j.vaccine.2017.08.089. Epub 2017 Sep 14. Vaccine. 2017. PMID: 28919226
-
Usefulness of specific IgG avidity for diagnosis of hepatitis A infection.Gastroenterol Clin Biol. 2005 May;29(5):573-6. doi: 10.1016/s0399-8320(05)82132-3. Gastroenterol Clin Biol. 2005. PMID: 15980754
-
Detection of hepatitis A virus RNA in serum during the window period of infection.J Clin Virol. 2004 Apr;29(4):254-9. doi: 10.1016/S1386-6532(03)00165-3. J Clin Virol. 2004. PMID: 15018853
-
Screening for hepatitis A and B antibodies in patients with chronic liver disease.Am J Med. 2005 Oct;118 Suppl 10A:28S-33S. doi: 10.1016/j.amjmed.2005.07.014. Am J Med. 2005. PMID: 16271538 Review.
-
Redefining the immune landscape of hepatitis A virus infection.Exp Mol Med. 2025 Apr;57(4):714-723. doi: 10.1038/s12276-025-01431-2. Epub 2025 Apr 2. Exp Mol Med. 2025. PMID: 40175697 Free PMC article. Review.
Cited by
-
Seroprevalence and Molecular Characterisation of Human Hepatitis A virus in Serum Samples of Tunisian Patients with Clinical Symptoms of Viral Hepatitis.Indian J Virol. 2012 Jun;23(1):29-35. doi: 10.1007/s13337-012-0063-6. Epub 2012 Mar 25. Indian J Virol. 2012. PMID: 23729999 Free PMC article.
-
Epidemiology of hepatitis A virus infections, Germany, 2007-2008.Emerg Infect Dis. 2009 Nov;15(11):1760-8. doi: 10.3201/eid1511.090214. Emerg Infect Dis. 2009. PMID: 19891863 Free PMC article.
-
Serum antibody response to Human papillomavirus (HPV) infections detected by a novel ELISA technique based on denatured recombinant HPV16 L1, L2, E4, E6 and E7 proteins.Infect Agent Cancer. 2006 Nov 8;1:6. doi: 10.1186/1750-9378-1-6. Infect Agent Cancer. 2006. PMID: 17150135 Free PMC article.
-
The potential significance of high avidity immunoglobulin G (IgG) for protective immunity towards SARS-CoV-2.Int J Infect Dis. 2021 May;106:61-64. doi: 10.1016/j.ijid.2021.01.061. Epub 2021 Mar 10. Int J Infect Dis. 2021. PMID: 33713819 Free PMC article.
-
Primary and probable secondary dengue virus (DV) infection rates in relation to age among DV IgM-positive patients residing in the United States mainland versus the Caribbean islands.Clin Vaccine Immunol. 2012 Jan;19(1):105-8. doi: 10.1128/CVI.05519-11. Epub 2011 Nov 23. Clin Vaccine Immunol. 2012. PMID: 22116685 Free PMC article.
References
-
- Aalto, S. M., K. Linnavuori, H. Peltola, E. Vuori, B. Weissbrich, J. Schubert, L. Hedman, and K. Hedman. 1998. Immunoreactivation of Epstein-Barr virus due to cytomegalovirus primary infection. J. Med. Virol. 56:186-191. - PubMed
-
- Andersson, A., V. Vetter, L. Kreutzer, and G. Bauer. 1994. Avidities of IgG directed against viral capsid antigen or early antigen: useful markers for significant Epstein-Barr virus serology. J. Med. Virol. 43:238-244. - PubMed
-
- Blackburn, N. K., T. G. Besselaar, B. D. Schoub, and K. F. O'Connell. 1991. Differentiation of primary cytomegalovirus infection from reactivation using the urea denaturation test for measuring antibody avidity. J. Med. Virol. 33:6-9. - PubMed
-
- Bower, W. A., O. V. Nainan, X. Han, and H. S. Margolis. 2000. Duration of viremia in hepatitis A virus infection. J. Infect. Dis. 182:12-17. - PubMed
-
- Castaneda-Ibarra, F., L. Ruiz-Maya, R. Campos-Rodriguez, and E. Garcia Latorre. 1991. Polyclonal activation of B lymphocytes in patients with amoebic hepatic abscess. Arch. Investig. Med. 22:13-17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
