

Surgical removal vs observation for subfoveal choroidal neovascularization, either associated with the ocular histoplasmosis syndrome or idiopathic: II. Quality-of-life findings from a randomized clinical trial: SST Group H Trial: SST Report No. 10
- PMID: 15534122
- PMCID: PMC1434792
- DOI: 10.1001/archopht.122.11.1616
Surgical removal vs observation for subfoveal choroidal neovascularization, either associated with the ocular histoplasmosis syndrome or idiopathic: II. Quality-of-life findings from a randomized clinical trial: SST Group H Trial: SST Report No. 10
Abstract
Objective: To report findings regarding health-related quality-of-life outcomes by treatment arm, both overall and within subgroups defined by selected baseline characteristics, among patients who participated in the Submacular Surgery Trials (SST) randomized trial of observation vs surgical removal of subfoveal choroidal neovascular lesions that were either idiopathic or associated with ocular histoplasmosis (SST Group H Trial).
Design and methods: Eligible patients were 18 years or older and had subfoveal choroidal neovascularization (including a classic component on fluorescein angiography) and visual acuity of 20/50 to 20/800 inclusive in the eye randomly assigned to surgery or observation. Trained interviewers, who were masked to treatment assignment, administered the National Eye Institute Visual Function Questionnaire (NEI-VFQ), the 36-Item Short-Form Health Survey (SF-36), and the Hospital Anxiety and Depression Scale (HADS) by telephone before enrollment and at 6, 12, and 24 months after enrollment; early enrollees also had interviews at 36 and 48 months. Baseline clinical examinations provided data regarding visual acuity, other aspects of vision, and presence of unilateral or bilateral choroidal neovascularization.
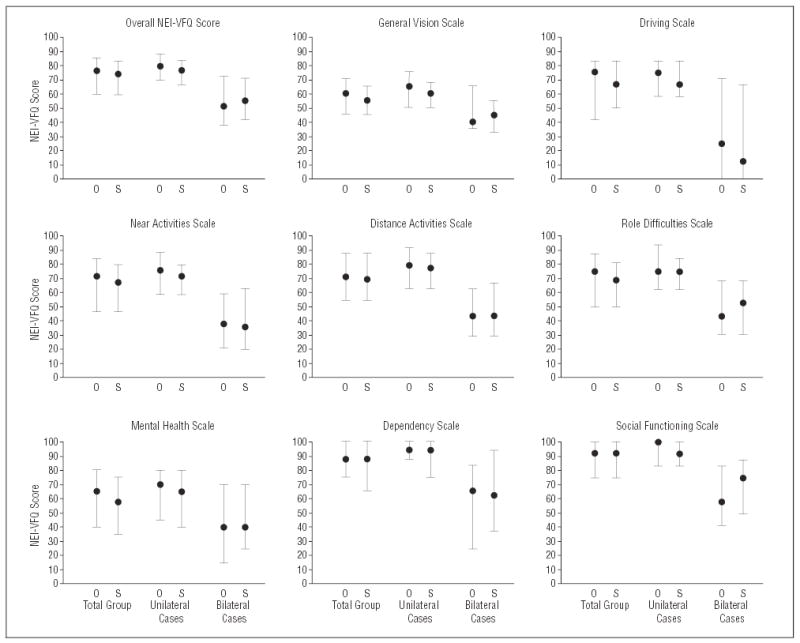
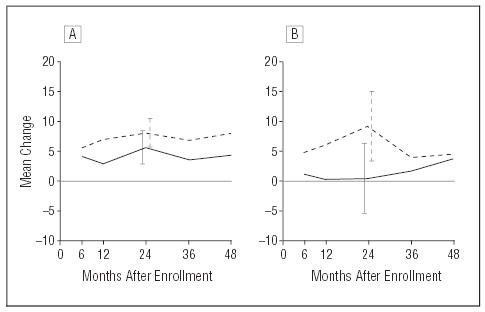
Results: Of 225 patients interviewed at baseline and enrolled, 201, 190, and 161 patients (respectively, 89%, 85%, and 88% of those eligible to be interviewed) were interviewed 12, 24, and 36 months later. The NEI-VFQ scores in both treatment arms improved from baseline (median score, 75) to the 24-month interview. Patients in the surgery arm had 4-point larger improvements, on average, than patients in the observation arm (95% confidence interval, 1-8 points). The largest differences between treatment arms for mean 24-month improvements from baseline were in the role difficulties subscale (9 points) and dependency subscale (8 points), with larger mean improvements in the surgery arm. Scores on the SF-36 worsened by approximately 1 point on the physical component summary and improved by 2 points or more on the mental component summary in both treatment arms by 24 months in comparison to baseline. The percentage of HADS-defined "definite cases" of both anxiety and depression declined from baseline in each treatment arm.
Conclusions: Vision-targeted quality of life improved more after submacular surgery than with observation, supporting a possible small overall benefit of surgery suggested by the ophthalmic outcomes reported elsewhere. Ophthalmologists and patients similar to those who participated in the SST Group H Trial should be aware of the effects of submacular surgery on specific aspects of vision-targeted quality of life as well as on ophthalmic outcomes when considering this treatment approach.
Figures



Comment in
-
Now that we have the results of the subretinal surgery trials, how do we manage the patient?Arch Ophthalmol. 2004 Nov;122(11):1705-6. doi: 10.1001/archopht.122.11.1705. Arch Ophthalmol. 2004. PMID: 15534134 No abstract available.
References
-
- Ware JE Jr. Evaluating measures of general health concepts for use in clinical trials. In: Furberg C, Schuttinga JA, eds. Quality of Life Assessment. Practice, Problems, and Promise: Proceedings of a Workshop, October 15–17, 1990. Washington, DC: US Dept of Health and Human Services; 1993:51–63. NIH publication 93–3503.
-
- Patrick DL. Reactions and recommendations: quality of life in NIH-sponsored studies. In: Furberg C, Schuttinga JA, eds. Quality of Life Assessment. Practice, Problems, and Promise. Proceedings of a Workshop, October 15–17, 1990. Washington, DC: US Dept of Health and Human Services; 1993:81–88. NIH publication 93–3503.
-
- Drummond MF, Ferris FF III. Major themes and conclusions: a strategy for measurement of quality of life in National Eye Institute Trials. In: Drummond MF, ed. Measuring the Quality of Life of People With Visual Impairment: Proceedings of a Workshop. Washington, DC: US Dept of Health and Human Services; 1990:65–66. NIH publication 90–3098.
-
- McDowell I. General health measurement and quality of life in visual impairment. In: Drummond MF, ed. Measuring the Quality of Life of People With Visual Impairment: Proceedings of a Workshop. Washington, DC: US Dept of Health and Human Services; 1990:29–33. NIH publication 90–3098.
-
- Submacular Surgery Trials Pilot Study Investigators. Submacular Surgery Trials randomized pilot trial of laser photocoagulation versus surgery for recurrent choroidal neovascularization secondary to age-related macular degeneration, II: Quality-of-life outcomes: Submacular Surgery Trials Pilot Study report No. 2. Am J Ophthalmol. 2000;130:408–418. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
