

Menopausal status dependence of the timing of breast cancer recurrence after surgical removal of the primary tumour
- PMID: 15535851
- PMCID: PMC1064084
- DOI: 10.1186/bcr937
Menopausal status dependence of the timing of breast cancer recurrence after surgical removal of the primary tumour
Abstract
Introduction: Information on the metastasis process in breast cancer patients undergoing primary tumour removal may be extracted from an analysis of the timing of clinical recurrence.
Methods: The hazard rate for local-regional and/or distant recurrence as the first event during the first 4 years after surgery was studied in 1173 patients undergoing mastectomy alone as primary treatment for operable breast cancer. Subset analyses were performed according to tumour size, axillary nodal status and menopausal status.
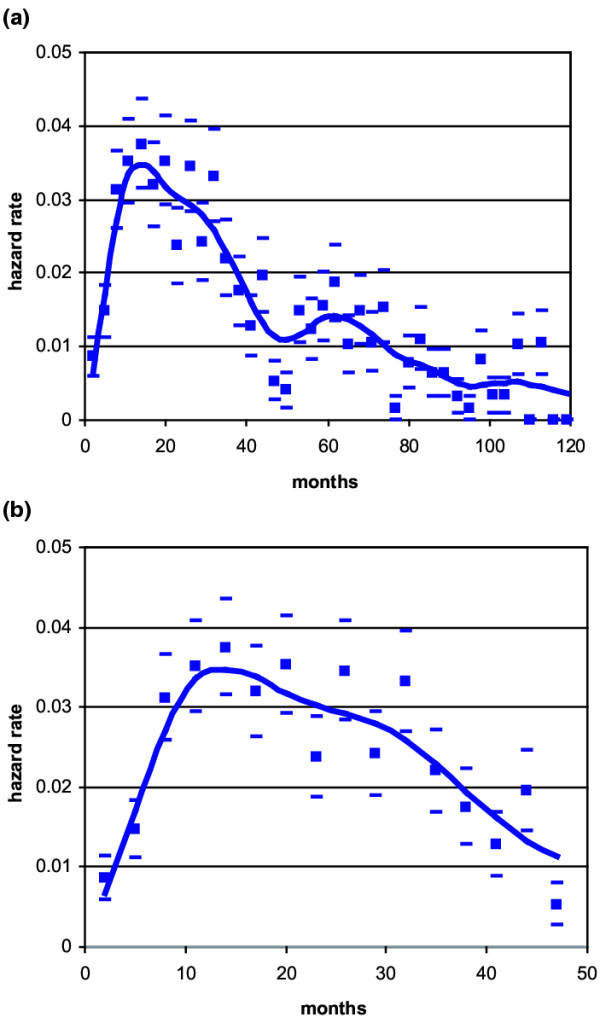
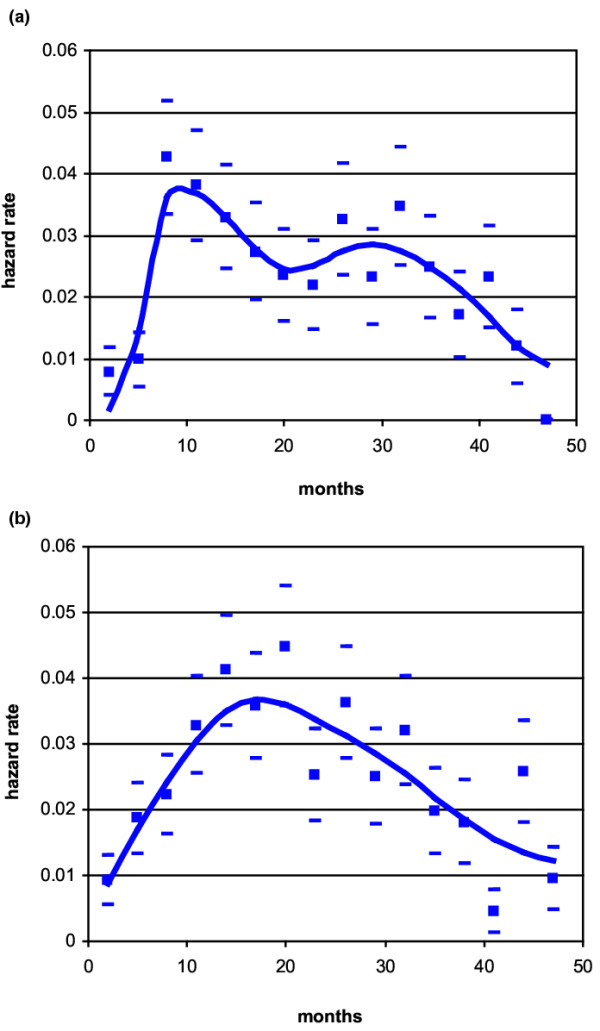
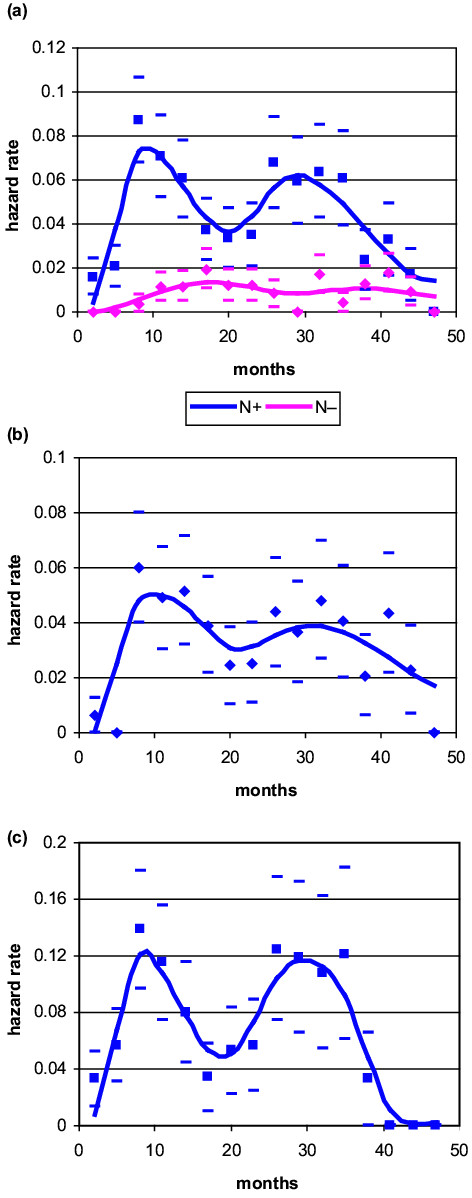
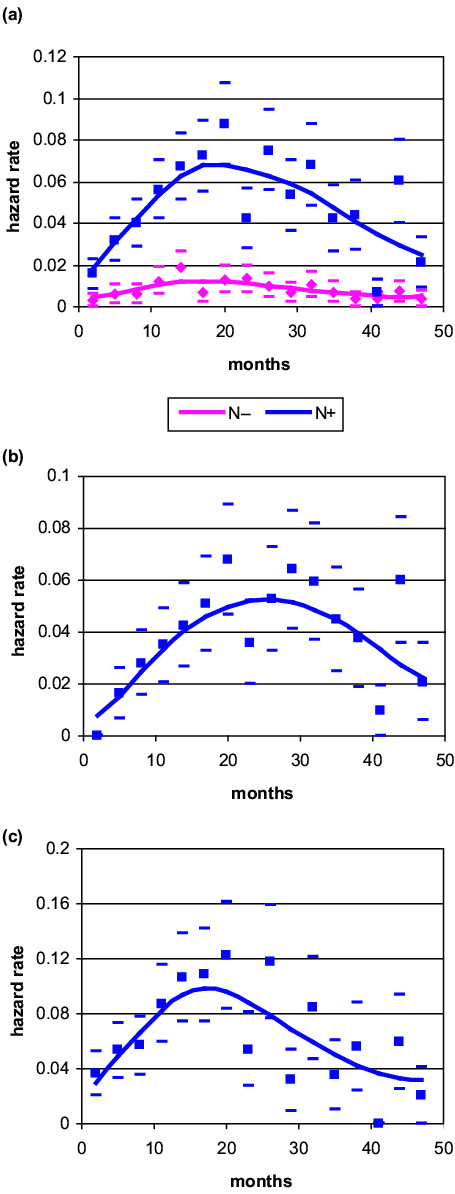
Results: A sharp two-peaked hazard function was observed for node-positive pre-menopausal patients, whereas results from node-positive post-menopausal women always displayed a single broad peak. The first narrow peak among pre-menopausal women showed a very steep rise to a maximum about 8-10 months after mastectomy. The second peak was considerably broader, reaching its maximum at 28-30 months. Post-menopausal patients displayed a wide, nearly symmetrical peak with maximum risk at about 18-20 months. Peaks displayed increasing height with increasing axillary lymph node involvement. No multi-peaked pattern was evident for either pre-menopausal or post-menopausal node-negative patients; however, this finding should be considered cautiously because of the limited number of events. Tumour size influenced recurrence risk but not its timing. Findings resulting from the different subsets of patients were remarkably coherent and each observed peak maintained the same position on the time axis in all analysed subsets.
Conclusions: The risk of early recurrence for node positive patients is dependent on menopausal status. The amount of axillary nodal involvement and the tumour size modulate the risk value at any given time. For pre-menopausal node-positive patients, the abrupt increase of the first narrow peak of the recurrence risk suggests a triggering event that synchronises early risk. We suggest that this event is the surgical removal of the primary tumour. The later, broader, more symmetrical risk peaks indicate that some features of the corresponding metastatic development may present stochastic traits. A metastasis development model incorporating tumour dormancy in specific micro-metastatic phases, stochastic transitions between them and sudden acceleration of the metastatic process by surgery can explain these risk dynamics.
Figures
Comment in
-
An early peak of relapse after surgery for breast cancer.Breast Cancer Res. 2004;6(6):255-7. doi: 10.1186/bcr946. Epub 2004 Oct 11. Breast Cancer Res. 2004. PMID: 15535855 Free PMC article.
References
-
- Fisher B, Carbone P, Economou SG, Frelick R, Glass A, Lerner H, Redmond C, Zelem M, Band P, Katrych DL, et al. 1-Phenylalanine mustard (L-PAM) in the management of primary breast cancer. A report of early findings. N Engl J Med. 1975;292:117–122. - PubMed
-
- Bonadonna G, Brusamolino E, Valagussa P, Rossi A, Brugnatelli L, Brambilla C, DeLena M, Tancini G, Bajetta E, Musumeci R, et al. Combination chemotherapy as an adjuvant treatment in operable breast cancer. N Engl J Med. 1976;294:405–410. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
