

Characterization of antibodies to capsular polysaccharide antigens of Haemophilus influenzae type b and Streptococcus pneumoniae in human immune globulin intravenous preparations
- PMID: 15539522
- PMCID: PMC524781
- DOI: 10.1128/CDLI.11.6.1158-1164.2004
Characterization of antibodies to capsular polysaccharide antigens of Haemophilus influenzae type b and Streptococcus pneumoniae in human immune globulin intravenous preparations
Abstract
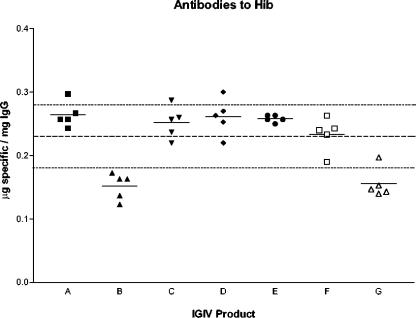
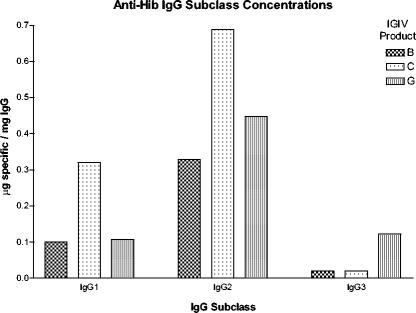
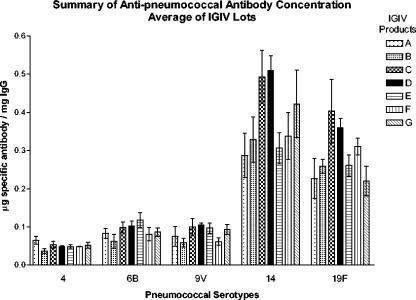
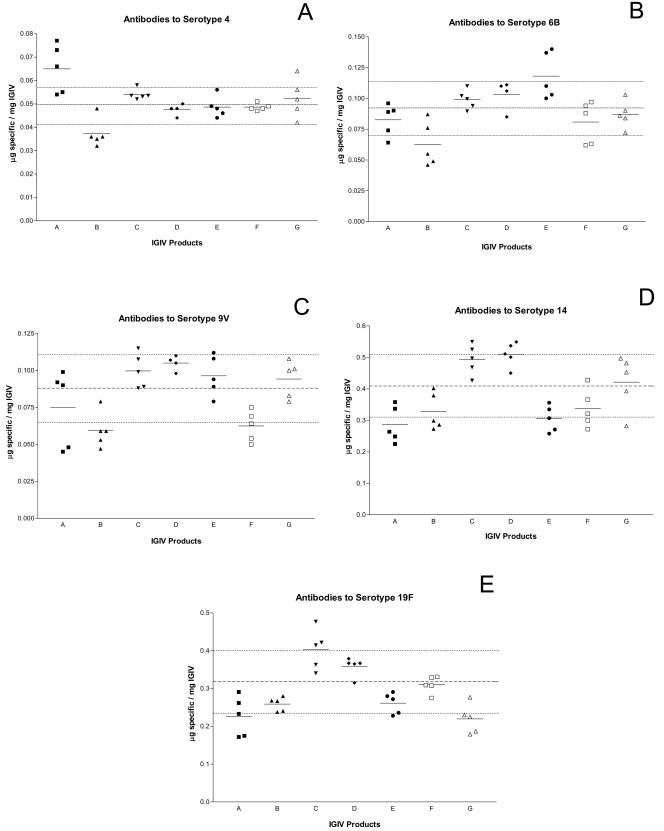
The most common infections in primary immune deficiency disease (PIDD) patients involve encapsulated bacteria, mainly Haemophilus influenzae type b (Hib) and Streptococcus pneumoniae (pneumococcus). Thus, it is important to know the titers of Hib- and pneumococcus-specific antibodies that are present in immune globulin (Ig) intravenous (IGIV) preparations used to treat PIDD. In this study, seven IGIV preparations were tested by enzyme-linked immunosorbent assay and opsonophagocytic activity for antibody titers to the capsular polysaccharides of Hib and five pneumococcal serotypes. Differences in Hib- and pneumococcus-specific antibody titer were observed among various IGIV preparations, with some products having higher- or lower-than-average titers. Opsonic activity also varied among preparations. As expected, IgG2 was the most active subclass of both binding and opsonic activity except against pneumococcal serotype 6B where IgG3 was the most active. This study determines antibody titers against capsular polysaccharides of Hib and pneumococcus in seven IGIV products that have been shown to be effective in reducing infections in PIDD patients. As donor antibody levels and manufacturing methods continue to change, it may prove useful from a regulatory point of view to reassess IGIV products periodically, to ensure that products maintain antibody levels that are important for the health of IGIV recipients.
Figures
Similar articles
-
Functional antibodies to Haemophilus influenzae type B, Neisseria meningitidis, and Streptococcus pneumoniae contained in intravenous immunoglobulin products.Transfusion. 2017 Jan;57(1):157-165. doi: 10.1111/trf.13869. Epub 2016 Oct 23. Transfusion. 2017. PMID: 27774610
-
Anti-capsular polysaccharide antibody deficiency states.Immunodeficiency. 1993;5(1):1-21. Immunodeficiency. 1993. PMID: 8167745 Review.
-
Consistency of protective antibody levels across lots of intravenous immunoglobulin preparations.J Allergy Clin Immunol. 2008 Jan;121(1):254-5. doi: 10.1016/j.jaci.2007.11.001. J Allergy Clin Immunol. 2008. PMID: 18206511 No abstract available.
-
Levels of antibodies specific to tetanus toxoid, Haemophilus influenzae type b, and pneumococcal capsular polysaccharide in healthy children and adults.Clin Diagn Lab Immunol. 2003 Mar;10(2):202-7. doi: 10.1128/cdli.10.2.202-207.2003. Clin Diagn Lab Immunol. 2003. PMID: 12626443 Free PMC article.
-
Global status of Haemophilus influenzae type b and pneumococcal conjugate vaccines: evidence, policies, and introductions.Curr Opin Infect Dis. 2010 Jun;23(3):236-41. doi: 10.1097/QCO.0b013e328338c135. Curr Opin Infect Dis. 2010. PMID: 20407316 Review.
Cited by
-
Streptococcus pneumoniae antibody titres in patients with primary antibody deficiency receiving intravenous immunoglobulin (IVIG) compared to subcutaneous immunoglobulin (SCIG).Clin Exp Immunol. 2015 Oct;182(1):51-6. doi: 10.1111/cei.12665. Epub 2015 Jul 29. Clin Exp Immunol. 2015. PMID: 26230522 Free PMC article. Clinical Trial.
-
Opsonophagocytic Antibodies to Serotype Ia, Ib, and III Group B Streptococcus among Korean Infants and in Intravenous Immunoglobulin Products.J Korean Med Sci. 2017 May;32(5):737-743. doi: 10.3346/jkms.2017.32.5.737. J Korean Med Sci. 2017. PMID: 28378545 Free PMC article.
-
Intravenous Immunoglobulin for Overwhelming Postsplenectomy Infection.J Glob Infect Dis. 2021 Jan 29;13(1):44-51. doi: 10.4103/jgid.jgid_93_19. eCollection 2021 Jan-Mar. J Glob Infect Dis. 2021. PMID: 33911454 Free PMC article.
-
Evaluation of a novel therapeutic approach to treating severe pneumococcal infection using a mouse model.Clin Vaccine Immunol. 2009 Jun;16(6):806-10. doi: 10.1128/CVI.00120-09. Epub 2009 Apr 22. Clin Vaccine Immunol. 2009. PMID: 19386795 Free PMC article.
-
Production of IgG antibodies to pneumococcal polysaccharides is associated with expansion of ICOS+ circulating memory T follicular-helper cells which is impaired by HIV infection.PLoS One. 2017 May 2;12(5):e0176641. doi: 10.1371/journal.pone.0176641. eCollection 2017. PLoS One. 2017. PMID: 28463977 Free PMC article.
References
-
- Asherson, G. L., and A. D. B. Webster (ed.). 1980. Diagnosis and treatment of immunodeficiency diseases. Blackwell, Oxford, United Kingdom.
-
- Ballow, M. 2002. Intravenous immunoglobulins: clinical experience and viral safety. J. Am. Pharm. Assoc. 42:449-458; quiz, 458-459. - PubMed
-
- Black, S., H. Shinefield, B. Fireman, E. Lewis, P. Ray, J. R. Hansen, L. Elvin, K. M. Ensor, J. Hackell, G. Siber, F. Malinoski, D. Madore, I. Chang, R. Kohberger, W. Watson, R. Austrian, K. Edwards et al. 2000. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Pediatr. Infect. Dis. J. 19:187-195. - PubMed
-
- Bridonneau, P., H. Marcilly, M. Vernois-Martin, P. Goigoux, V. Bourdel, A. Laulan, F. X. Deramoudt, M. Desmadril, M. Sitbon, B. Basuyaux, M. Steinbuch, and R. Schmitthaeusler. 1996. Liquid pasteurization of an immunoglobulin preparation without stabilizer: effects on its biological and biochemical properties. Vox Sang. 70:203-209. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
