

Helicobacter pylori test and eradicate versus prompt endoscopy for management of dyspeptic patients: 6.7 year follow up of a randomised trial
- PMID: 15542510
- PMCID: PMC1774341
- DOI: 10.1136/gut.2004.043570
Helicobacter pylori test and eradicate versus prompt endoscopy for management of dyspeptic patients: 6.7 year follow up of a randomised trial
Abstract
Background: Dyspepsia is a chronic disease with significant impact on the use of health care resources. A management strategy based on Helicobacter pylori testing has been recommended but the long term effect is unknown.
Aim: To investigate the long term effect of a test and treat strategy compared with prompt endoscopy for management of dyspeptic patients in primary care.
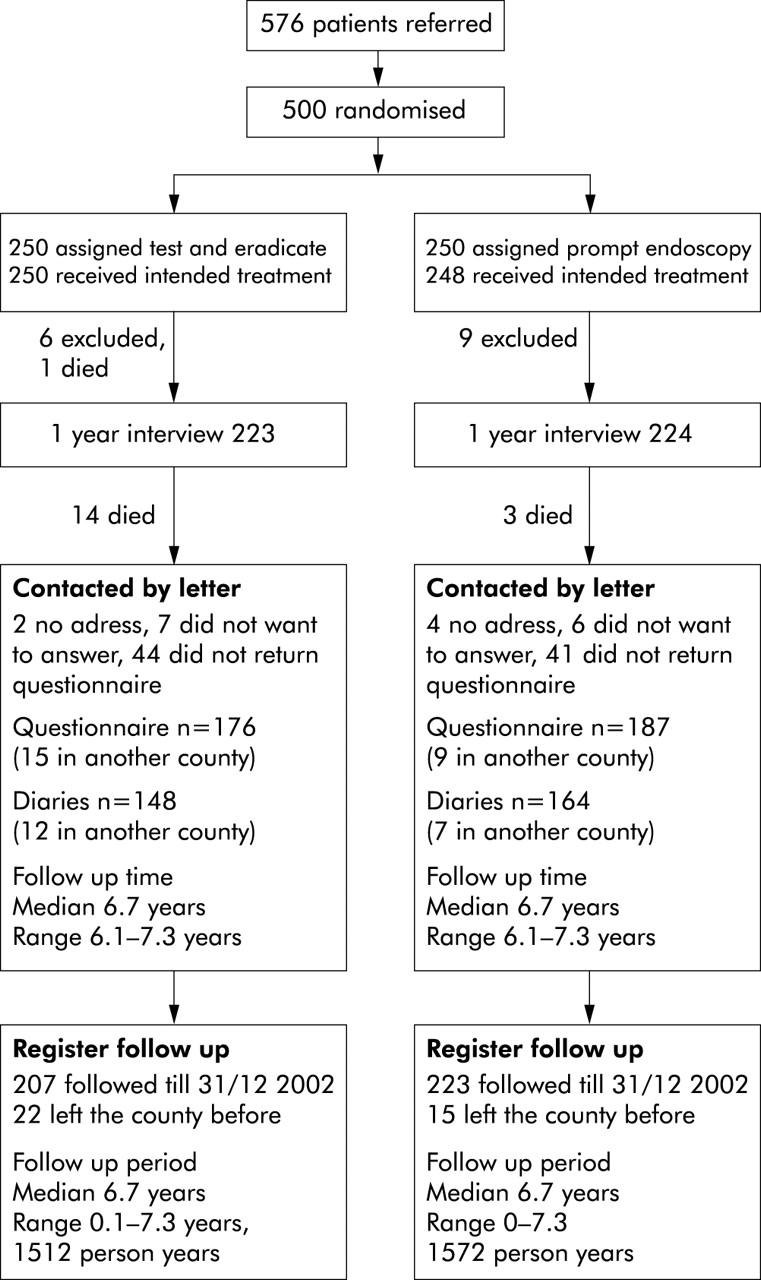
Patients: A total of 500 patients presenting in primary care with dyspepsia were randomised to management by H pylori testing plus eradication therapy (n = 250) or by endoscopy (n = 250). Results of 12 month follow up have previously been presented.
Methods: Symptoms, quality of life, and patient satisfaction were recorded during a three month period, a median 6.7 years after randomisation (range 6.1-7.3 years). Number of endoscopies, antisecretory medication, H pylori treatments, and hospital visits were recorded from health care databases for the entire follow up period.
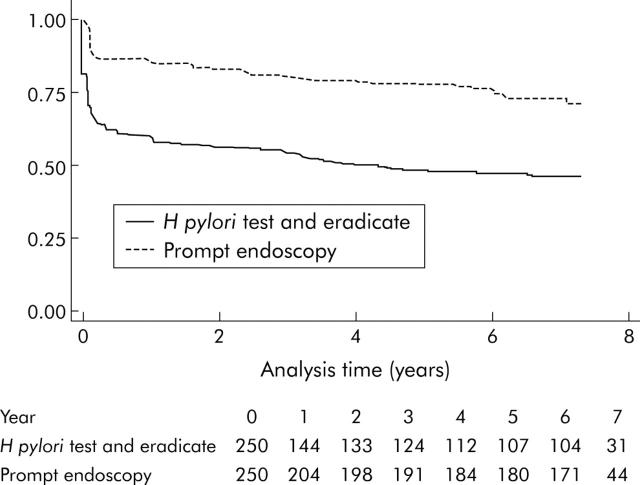
Results: Median age was 45 years; 28% were H pylori infected. Use of resources was registered in all 500 patients (3084 person years) of whom 312 completed diaries. We found no difference in symptoms between the two groups. Median proportion of days without symptoms was 0.52 (interquartile range 0.10-0.88) in the test and eradicate group versus 0.64 (0.14-0.90) in the prompt endoscopy group (p = 0.27) (mean difference 0.05 (95% confidence interval (CI) -0.03 to 0.14)). Compared with the prompt endoscopy group, the test and eradicate group underwent fewer endoscopies (mean difference 0.62 endoscopies/person (95% CI 0.38-0.86)) and used less antisecretory medication (mean difference 102 defined daily doses/person (95% CI -1 to 205)).
Conclusion: On a long term basis, a H pylori test and eradicate strategy is as efficient as prompt endoscopy for management of dyspeptic patients in primary care and reduces the use of endoscopy and antisecretory medication.
Figures
Comment in
-
Helicobacter pylori test-and-eradicate strategy versus early endoscopy in patients with dyspepsia.Nat Clin Pract Gastroenterol Hepatol. 2005 Feb;2(2):70-1. doi: 10.1038/ncpgasthep0091. Nat Clin Pract Gastroenterol Hepatol. 2005. PMID: 16265119 No abstract available.
References
-
- Delaney BC, Moayyedi P, Forman D. Initial management strategies for dyspepsia. Cochrane Database Syst Rev 2003:CD001961. - PubMed
-
- Talley NJ, Silverstein MD, Agreus L, et al. AGA technical review: evaluation of dyspepsia. American Gastroenterological Association. Gastroenterology 1998;114:582–95. - PubMed
-
- Malfertheiner P , Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection—the Maastricht 2-2000 Consensus Report. Aliment Pharmacol Ther 2002;16:167–80. - PubMed
-
- Fendrick AM, Chernew ME, Hirth RA, et al. Alternative management strategies for patients with suspected peptic ulcer disease. Ann Intern Med 1995;123:260–8. - PubMed
-
- Ladabaum U , Chey WD, Scheiman JM, et al. Reappraisal of non-invasive management strategies for uninvestigated dyspepsia: a cost-minimization analysis. Aliment Pharmacol Ther 2002;16:1491–501. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical