

Acetylated sialic acid residues and blood group antigens localise within the epithelium in microvillous atrophy indicating internal accumulation of the glycocalyx
- PMID: 15542511
- PMCID: PMC1774315
- DOI: 10.1136/gut.2004.041954
Acetylated sialic acid residues and blood group antigens localise within the epithelium in microvillous atrophy indicating internal accumulation of the glycocalyx
Abstract
Background: Microvillous atrophy, a disorder of intractable diarrhoea in infancy, is characterised by the intestinal epithelial cell abnormalities of abnormal accumulation of periodic acid-Schiff (PAS) positive secretory granules within the apical cytoplasm and the presence of microvillous inclusions. The identity of the PAS positive material is not known, and the aim of this paper was to further investigate its composition.
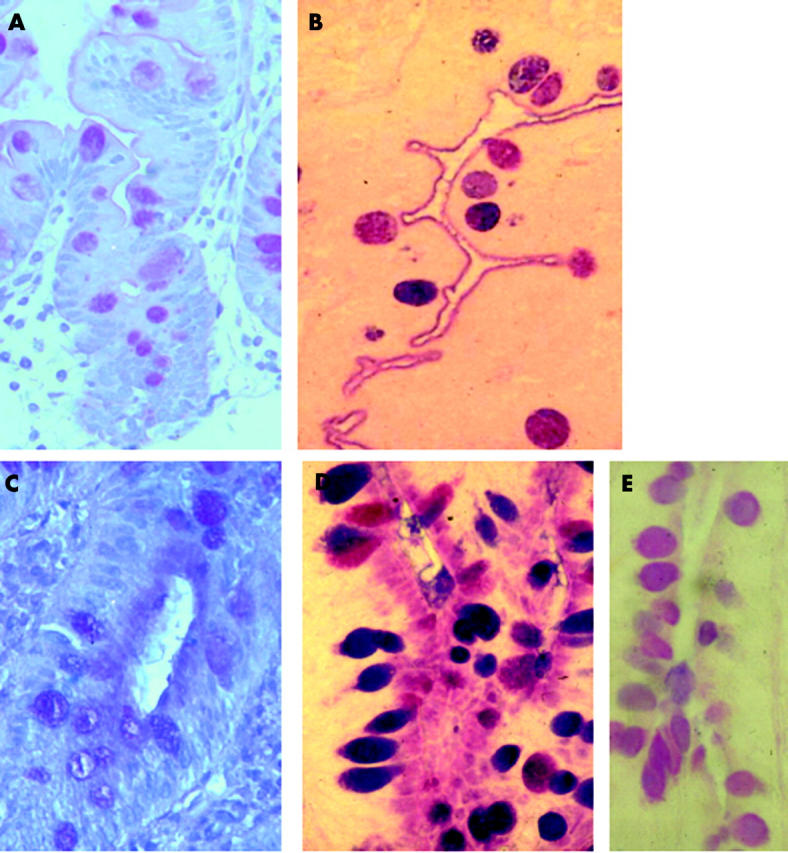
Methods: Formaldehyde fixed sections were stained with alcian blue/PAS to identify the acidic or neutral nature of the material, phenylhydrazine blocking was employed to stain specifically for sialic acid, and saponification determined the presence of sialic acid acetylation. The specificity of sialic acid staining was tested by digestion with mild sulphuric acid. Expression of blood group related antigens was tested immunochemically.
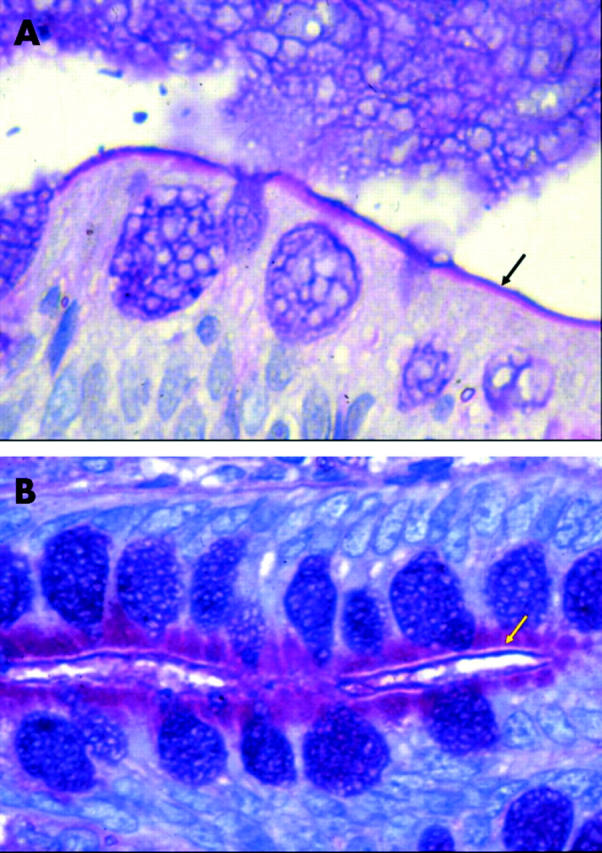
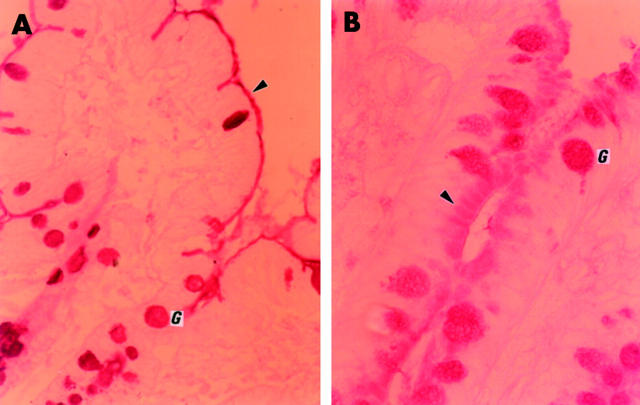
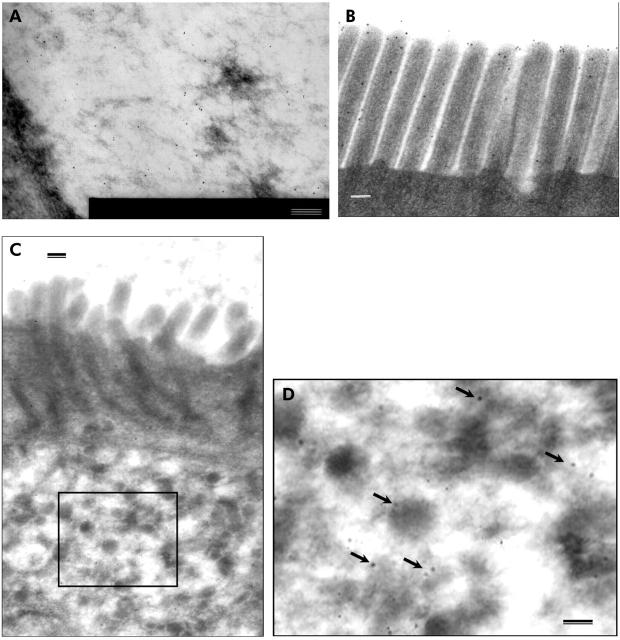
Results: Alcian blue/PAS staining identified a closely apposed layer of acidic material on the otherwise neutral (PAS positive) brush border in controls. In microvillous atrophy, a triple layer was seen with an outer acidic layer, an unstained brush border region, and accumulation within the epithelium of a neutral glycosubstance that contained acetylated sialic acid. Blood group antigens were detected on the brush border, in mucus, and within goblet cells in controls. In microvillous atrophy they were additionally expressed within the apical cytoplasm of epithelial cells mirroring the PAS abnormality. Immuno electron microscopy localised expression to secretory granules.
Conclusions: A neutral, blood group antigen positive, glycosubstance that contains acetylated sialic acid accumulates in the epithelium in microvillous atrophy. Previous studies have demonstrated that the direct and indirect constitutive pathways are intact in this disorder and it is speculated that the abnormal staining pattern reflects accumulation of glycocalyx related material.
Figures

References
-
- Phillips AD, Schmitz J. Familial microvillous atrophy: a clinicopathological survey of 23 cases. J Pediatr Gastroenterol Nutr 1992;14:380–96. - PubMed
-
- Schofield DE, Agostini RM, Yunis M. Gastrointestinal microvillus inclusion disease. Am J Clin Pathol 1992;98:119–24. - PubMed
-
- Herzog D , Atkinson P, Grant D, et al. Combined bowel-liver transplantation in an infant with microvillus inclusion disease. J Pediatr Gastroenterol Nutr 1996;22:405–8. - PubMed
-
- Oliva M , Perman JA, Saavedra JM, et al. Successful intestinal transplantation for microvillus inclusion disease. Gastroenterol 1994;106:771–4. - PubMed
-
- Randak C , Langnas AN, Kaufman SS, et al. Pretransplant management and small bowel-liver transplantation in an infant with microvillus inclusion disease. J Pediatr Gastroenterol Nutr 1998;27:333–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources