

Reassessment of diagnostic criteria in cutaneous lymphocytic infiltrates
- PMID: 15543371
- PMCID: PMC11126165
- DOI: 10.1590/s1516-31802004000400006
Reassessment of diagnostic criteria in cutaneous lymphocytic infiltrates
Abstract
Context: Non-specific lymphocytic infiltrates of the skin pose difficulties in daily practice in pathology. There is still a lack of pathognomonic signs for the differential diagnosis between benign and malignant lymphocytic infiltrates.
Objective: To evaluate the morphological and immunohistochemical profile of lymphocytic infiltrations of the skin according to clinical outcome.
Type of study: Retrospective; histopathological and immunohistochemical analysis.
Setting: Referral center, university hospital.
Sample: 28 cases of lymphocytic infiltrates of difficult differential diagnosis selected from the records.
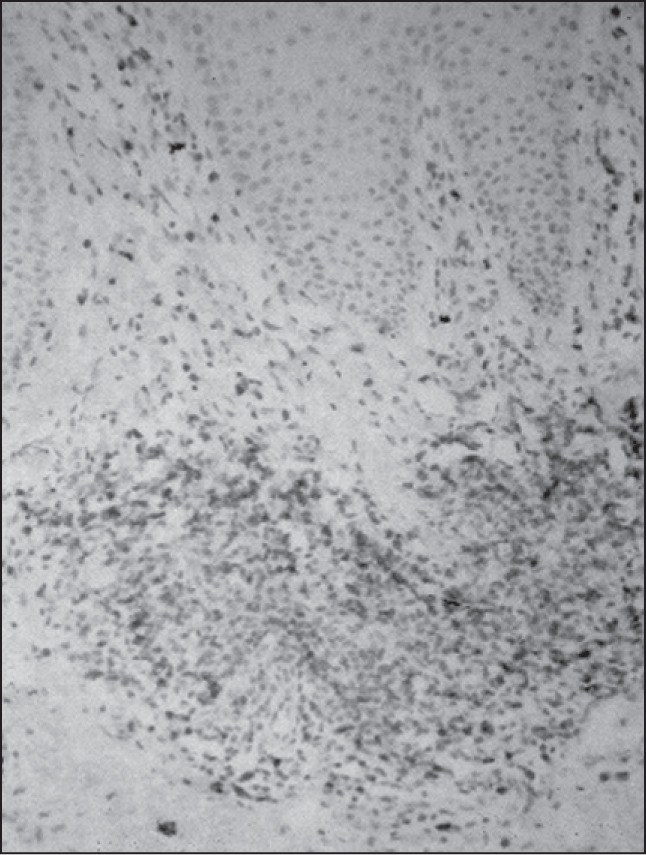
Main measurements: Eighteen histological variables and the immunophenotypic profile were assessed using the CD4, CD8, CD3, CD20 and CD30 lymphoid markers and compared to subsequent follow-up.
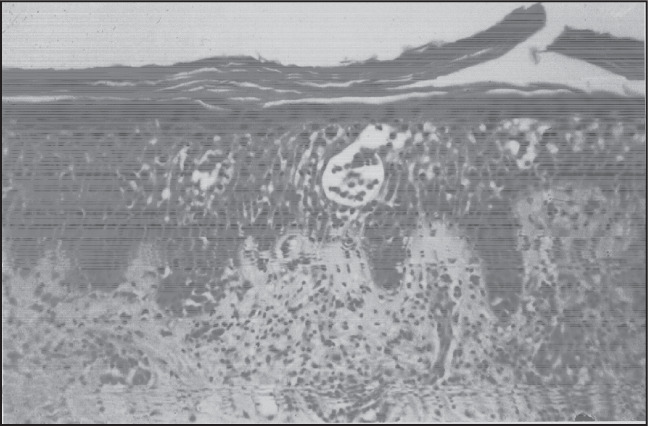
Results: The most common diagnoses were: initial mycosis fungoides (eight cases) and drug reactions (five cases). Single morphological variables did not discriminate between benign and malignant infiltrates except for the presence of Pautrier-Darier's microabscesses, which were found only in mycosis fungoides (p = 0.015). Patterns of superficial and deep infiltration (p = 0.037) and also the presence of eosinophils (p = 0.0207) were more frequently found in benign lymphocytic infiltrates. Immunohistochemical profile of T-cell subsets showed overlap between benign and malignant infiltrates with a predominance of CD4-positive (helper) lymphocytes in the majority of cases.
Conclusions: A combination of clinical and histological features remains the most reliable approach for establishing a definite diagnosis in cases of lymphoid skin infiltrates.
CONTEXTO:: Infiltrações linfocitárias não-específicas da pele representam dificuldades diagnósticas na prática diária da patologia. Não há sinais patognomônicos para o diagnóstico diferencial entre infiltrações linfocitárias benignas e malignas.
OBJETIVOS:: Avaliar o perfil morfológico e imunofenotípico das infiltrações linfocitárias de acordo com a evolução clínica.
TIPO DE ESTUDO:: Retrospectivo: análise histopatológica e imunoistoquímica.
LOCAL:: Centro de referência, hospital universitário.
AMOSTRA:: 28 casos de infiltrações linfocitárias de diagnóstico diferencial difícil selecionados dos arquivos.
PRINCIPAIS MEDIDAS:: Análise de 18 variáveis histológicas e perfil imunofenotípico utilizando os marcadores linfóides CD4, CD8, CD3, CD20 e CD30, comparados à evolução clínica.
RESULTADOS:: Os diagnósticos mais comuns foram: micose fungóide — inicial (oito casos) e farmacodermias (cinco casos). Variáveis morfológicas isoladas não discriminaram infiltrados benignos e malignos, exceto pela presença dos microabscessos de PautrierDarier, que foram encontrados apenas na micose fungóide (p = 0,015). O padrão de infiltração superficial e profunda (p = 0,037) e a presença de eosinófilos (p = 0,0207) foram mais freqüentes nas infiltrações linfocitárias benignas. O perfil imunoistoquímico dos linfócitos T mostrou sobreposição entre infiltrações benignas e malignas, com predomínio de linfócitos T auxiliares CD4 positivos na maioria dos casos.
CONCLUSÃO:: A combinação das informações clínicas e histológicas representa a abordagem mais consistente para o diagnóstico diferencial dos infiltrados linfóides cutâneos.
Figures

Similar articles
-
Immunohistochemical analysis of mycosis fungoides on paraffin-embedded tissue sections.Mod Pathol. 1998 Oct;11(10):978-82. Mod Pathol. 1998. PMID: 9796726
-
Comparison between the histopathological and immunophenotypical features of hypopigmented and nonhypopigmented mycosis fungoides: A retrospective study.J Cutan Pathol. 2021 Apr;48(4):486-494. doi: 10.1111/cup.13882. Epub 2020 Oct 29. J Cutan Pathol. 2021. PMID: 32965737
-
Adult pityriasis lichenoides-like mycosis fungoides: a clinical variant of mycosis fungoides.Int J Dermatol. 2014 Nov;53(11):1331-8. doi: 10.1111/ijd.12135. Epub 2014 Jun 25. Int J Dermatol. 2014. PMID: 24961281
-
[Mycosis fungoides or inflammatory dermatitis: differential diagnosis between early lymphoma and inflammation in skin biopsies].Pathologe. 2013 May;34(3):215-24. doi: 10.1007/s00292-013-1744-7. Pathologe. 2013. PMID: 23549914 Review. German.
-
[Mycosis fungoides in children and adolescents: a report of six cases with predominantly hypopigmentation, along with a literature review].Dermatol Online J. 2012 Mar 15;18(3):5. Dermatol Online J. 2012. PMID: 22483516 Review. Portuguese.
Cited by
-
Origin Use of CD4, CD8, and CD1a Immunostains in Distinguishing Mycosis Fungoides from its Inflammatory Mimics: A Pilot Study.Indian J Dermatol. 2012 Nov;57(6):424-7. doi: 10.4103/0019-5154.103060. Indian J Dermatol. 2012. PMID: 23248358 Free PMC article.
-
Approach to Cutaneous Lymphoid Infiltrates: When to Consider Lymphoma?Indian J Dermatol. 2016 Jul-Aug;61(4):351-74. doi: 10.4103/0019-5154.185698. Indian J Dermatol. 2016. PMID: 27512181 Free PMC article. Review.
References
-
- Elder D, Elenitsas R, Jawarsky C, Johnson B. Lever's Histopathology of the Skin. 8 edition. Philadelphia: Lippincott-Raven; 1997.
-
- Weedon D. Skin Pathology. London: Churchill Livingstone; 1997.
-
- Ming M, LeBoit PE. Can dermatopathologists reliably make the diagnosis of mycosis fungoides? If not, who can? Arch Dermatol. 2000;136(4):543–546. - PubMed
-
- Santucci M, Biggeri A, Feller AC, Massi D, Burg G. Efficacy of histologic criteria for diagnosing early mycosis fungoides: an EORTC cutaneous lymphoma study group investigation. European Organization for Research and Treatment of Cancer. Am J Surg Pathol. 2000;24(1):40–50. - PubMed
-
- Ackerman AB. Histologic Diagnosis of Inflammatory Skin Diseases. 2 edition. Baltimore: Williams & Wilkins; 1997.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
