

How does trust affect patient preferences for participation in decision-making?
- PMID: 15544684
- PMCID: PMC5060263
- DOI: 10.1111/j.1369-7625.2004.00296.x
How does trust affect patient preferences for participation in decision-making?
Abstract
Objective: Does trust in physicians aid or hinder patient autonomy? We examine the relationship between trust in the recipient's doctor, and desire for a participative role in decisions about medical treatment.
Design: We conducted a cross-sectional survey in an urban Canadian teaching hospital.
Setting and participants: A total of 606 respondents in three clinics (breast cancer, prostate cancer, fracture) completed questionnaires.
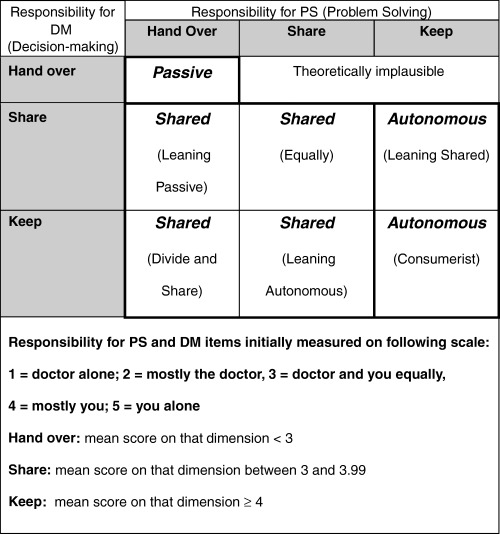
Variables studied: The instrument included the Problem Solving Decision Making (PSDM) Scale, which used two vignettes (current health condition, chest pain) to categorize respondents by preferred role, and the Trust-in-Physician Scale.
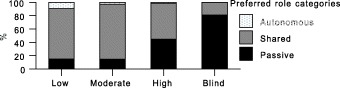
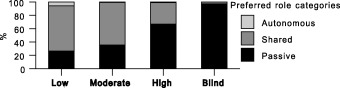
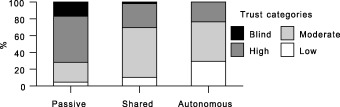
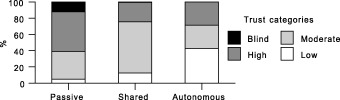
Results: Few respondents preferred an autonomous role (2.9% for the current health condition vignette and 1.2% for the chest pain vignette); most preferred shared decision-making (DM) (67.3% current health condition; 48.7% chest pain) or a passive role (29.6% current health condition; 50.1% chest pain). Trust-in-physician yielded 6.3% with blind trust, 36.1% with high trust, 48.6% moderate trust and 9.0% low trust. As hypothesized, autonomous patients had relatively low levels of trust, passive respondents were more likely to have blind trust, while shared respondents had high but not excessive trust. Trust had a significant influence on preferred role even after controlling for the demographic factors such as sex, age and education.
Conclusions: Very few respondents wish an autonomous role; those who do tend to have lower trust in their providers. Familiarity with a clinical condition increases desire for a shared (as opposed to passive) role. Shared DM often accompanies, and may require, a trusting patient-physician relationship.
Figures
Comment in
-
Trust and shared decision-making: an emerging research agenda.Health Expect. 2004 Dec;7(4):271-3. doi: 10.1111/j.1369-7625.2004.00304.x. Health Expect. 2004. PMID: 15544680 Free PMC article. No abstract available.
References
-
- President's Commission . President's Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Making Health Care Decisions: The Ethical and Legal Implications of Informed Consent in the Patient‐Practitioner Relationship, Vol. 1. Washington, DC: Government Printing Office, 1982.
-
- Katz J. The Silent World of Doctor and Patient. New York: Free Press, 1984.
-
- Beauchamp TL, Childress JF. Principles of Biomedical Ethics. New York, Oxford: Oxford University Press, 1989.
-
- Kassirer JP. Incorporating patients’ preferences into medical decisions. New England Journal of Medicine, 1994; 330: 1895–1896. - PubMed
-
- Pellegrino ED. Patient and physician autonomy: conflicting rights and obligations in the physician–patient relationship. Journal of Contemporary Health Law and Policy, 1994; 10: 47–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
