

Tregs and allergic disease
- PMID: 15545986
- PMCID: PMC525754
- DOI: 10.1172/JCI23595
Tregs and allergic disease
Abstract
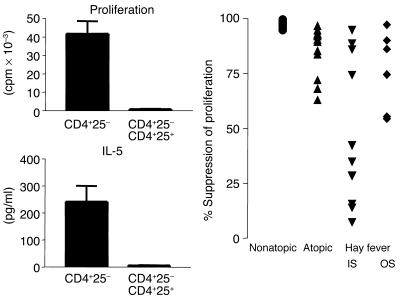
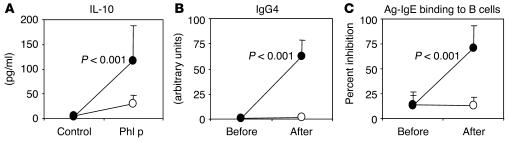
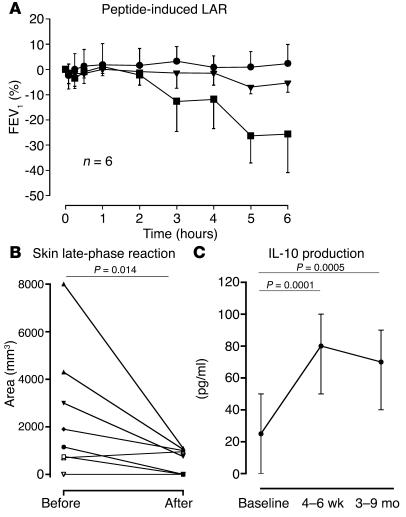
Allergic diseases such as asthma, rhinitis, and eczema are increasing in prevalence and affect up to 15% of populations in Westernized countries. The description of Tregs as T cells that prevent development of autoimmune disease led to considerable interest in whether these Tregs were also normally involved in prevention of sensitization to allergens and whether it might be possible to manipulate Tregs for the therapy of allergic disease. Current data suggest that Th2 responses to allergens are normally suppressed by both CD4+CD25+ Tregs and IL-10 Tregs. Furthermore, suppression by these subsets is decreased in allergic individuals. In animal models, Tregs could be induced by high- or low-dose inhaled antigen, and prior induction of such Tregs prevented subsequent development of allergen sensitization and airway inflammation in inhaled challenge models. For many years, allergen-injection immunotherapy has been used for the therapy of allergic disease, and this treatment may induce IL-10 Tregs, leading to both suppression of Th2 responses and a switch from IgE to IgG4 antibody production. Improvements in allergen immunotherapy, such as peptide therapy, and greater understanding of the biology of Tregs hold great promise for the treatment and prevention of allergic disease.
Figures

Similar articles
-
Regulatory T cells and asthma.Clin Exp Allergy. 2009 Sep;39(9):1314-23. doi: 10.1111/j.1365-2222.2009.03301.x. Epub 2009 Jun 17. Clin Exp Allergy. 2009. PMID: 19538496 Review.
-
Foxp3 expressing regulatory T-cells in allergic disease.Adv Exp Med Biol. 2009;665:180-94. doi: 10.1007/978-1-4419-1599-3_14. Adv Exp Med Biol. 2009. PMID: 20429425 Review.
-
CD4+CD25+ Regulatory T Cells Decreased CD8+IL-4+Cells in a Mouse Model of Allergic Asthma.Iran J Allergy Asthma Immunol. 2019 Aug 17;18(4):369-378. doi: 10.18502/ijaai.v18i4.1415. Iran J Allergy Asthma Immunol. 2019. PMID: 31522445
-
Sensitization to common allergens and its association with allergic disorders at age 4 years: a whole population birth cohort study.Pediatrics. 2001 Aug;108(2):E33. doi: 10.1542/peds.108.2.e33. Pediatrics. 2001. PMID: 11483843
-
CD25+ T cells and regulation of allergen-induced responses.Curr Allergy Asthma Rep. 2005 Jan;5(1):35-41. doi: 10.1007/s11882-005-0052-6. Curr Allergy Asthma Rep. 2005. PMID: 15659261 Review.
Cited by
-
Mechanisms of Particles in Sensitization, Effector Function and Therapy of Allergic Disease.Front Immunol. 2020 Jun 30;11:1334. doi: 10.3389/fimmu.2020.01334. eCollection 2020. Front Immunol. 2020. PMID: 32714326 Free PMC article. Review.
-
Autoimmune Pancreatitis: From Pathogenesis to Treatment.Int J Mol Sci. 2022 Oct 21;23(20):12667. doi: 10.3390/ijms232012667. Int J Mol Sci. 2022. PMID: 36293522 Free PMC article. Review.
-
Local nasal specific immunotherapy for allergic rhinitis.Allergy Asthma Clin Immunol. 2006 Sep 15;2(3):117-23. doi: 10.1186/1710-1492-2-3-117. Epub 2006 Sep 15. Allergy Asthma Clin Immunol. 2006. PMID: 20525156 Free PMC article.
-
Regulatory T Cells, a Potent Immunoregulatory Target for CAM Researchers: Modulating Allergic and Infectious Disease Pathology (II).Evid Based Complement Alternat Med. 2006 Jun;3(2):209-15. doi: 10.1093/ecam/nel020. Epub 2006 Apr 19. Evid Based Complement Alternat Med. 2006. PMID: 16786050 Free PMC article.
-
Selective IgA Deficiency and Allergy: A Fresh Look to an Old Story.Medicina (Kaunas). 2022 Jan 15;58(1):129. doi: 10.3390/medicina58010129. Medicina (Kaunas). 2022. PMID: 35056437 Free PMC article. Review.
References
-
- Kay AB. Allergy and allergic diseases. N. Engl. J. Med. 2001;344:30–37. - PubMed
-
- Lloyd CM, Gonzalo JA, Coyle AJ, Gutierrez-Ramos JC. Mouse models of allergic airway disease. Adv. Immunol. 2001;77:263–295. - PubMed
-
- Robinson DS. Th-2 cytokines in allergic disease. Br. Med. Bull. 2000;56:956–968. - PubMed
-
- Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. J. Immunol. 1995;155:1151–1164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
