

Review
doi: 10.1136/hrt.2004.041798.
Pathologic assessment of the vulnerable human coronary plaque
Affiliations
- PMID: 15547008
- PMCID: PMC1768577
- DOI: 10.1136/hrt.2004.041798
Item in Clipboard
Review
Pathologic assessment of the vulnerable human coronary plaque
Heart.
2004 Dec.
No abstract available
Figures
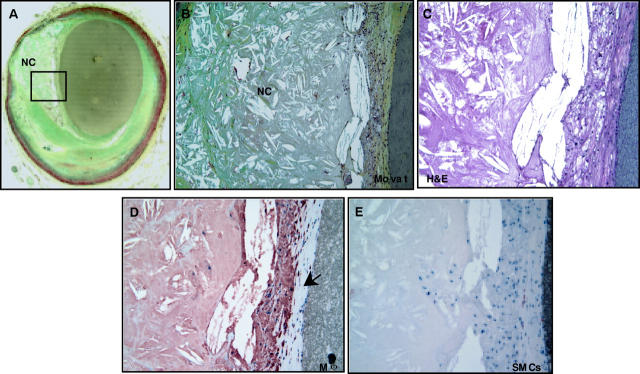
A non-haemodynamically limiting thin cap fibroatheroma. (A) Low power view of a thin cap fibroatheroma (TCFA) with a relatively large eccentric necrotic core (NC) and an overlying thin fibrous cap (< 65 μm); the greyish material in the lumen is barium gelatin (Movat pentachrome, ×20). (B) Image of the boxed area in panel A showing an advanced necrotic core with a loss of matrix containing numerous cholesterol clefts and cellular debris (×100). (C) High power view of a fibrous cap heavily infiltrated by inflammatory cells (haematoxylin and eosin, ×200). (D) Numerous CD-68 positive macrophages are localised to the fibrous cap (×200). (E) The fibrous cap shows rare α-actin positive smooth muscle cells (SMCs) (×200).
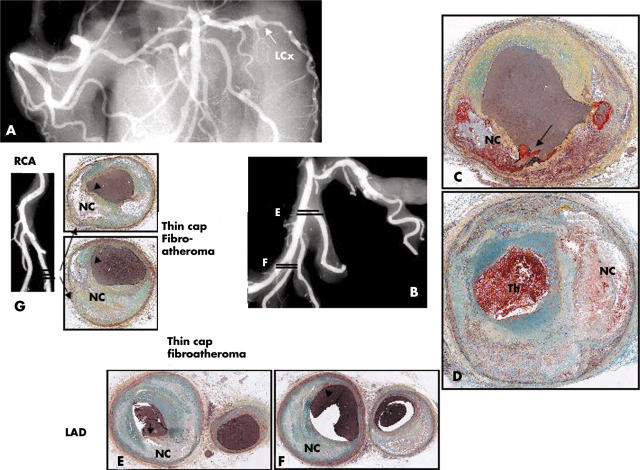
Plaque rupture in a 43 year old white male who collapsed at work and could not be resuscitated. The patient had recent complaints of shoulder pain and headache but no known medical history or risk factors. At necropsy there was haemopericardium with 500 ml of blood and a long vertical tear on the posterolateral surface of the left ventricle. There was an acute transmural myocardial infarction in the lateral wall of the left ventricle and a haemorrhagic tract in the area of the rupture, which was located in the middle of the infarct. The myocardium showed coagulation necrosis with prominent neutrophilic infiltrate consistent with a 2–3 day old infarct. A postmortem angiogram showed total occlusion of the left circumflex (LCx) artery (arrow in A and B). Histologic sections demonstrate fibrous cap rupture (arrow in C) with underlying hemorrhagic necrosis (NC). (D) Just distal to the site of rupture the coronary artery there is approximately 70% diameter stenosis and an overlying occlusive thrombus. (E) Sections of the first diagonal and LAD (E) and the distal third diagonal (F) show fibrous cap thinning with mild insignificant luminal narrowing and positive remodelling. (G) The angiogram of the distal right coronary artery (RCA) and the PDA shows mild irregularities at the site of sectioning, shown in dark lines. Note sites of fibrous cap thinning (arrows) overlying relatively larger necrotic cores (NC).
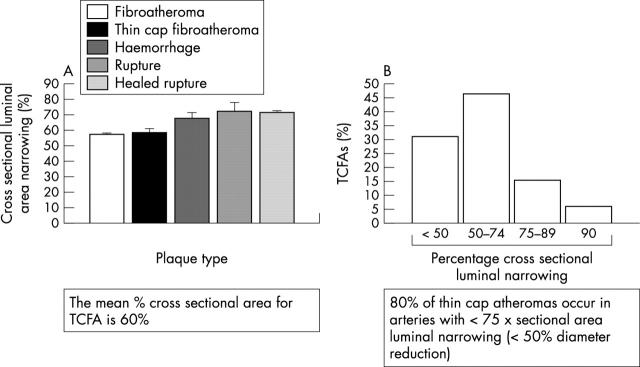
Morphometric analysis of thin-cap fibroatheromas. (A) Shows the percentage of cross sectional area luminal narrowing by plaque type. The thin cap fibroatheromas (TCFAs) and fibroatheromas are less narrowed than acute or healed ruptures. (B) The percentage of TCFAs are plotted against the degree of luminal narrowing. Notably, over 80% of these lesions have < 75% cross sectional area luminal narrowing.
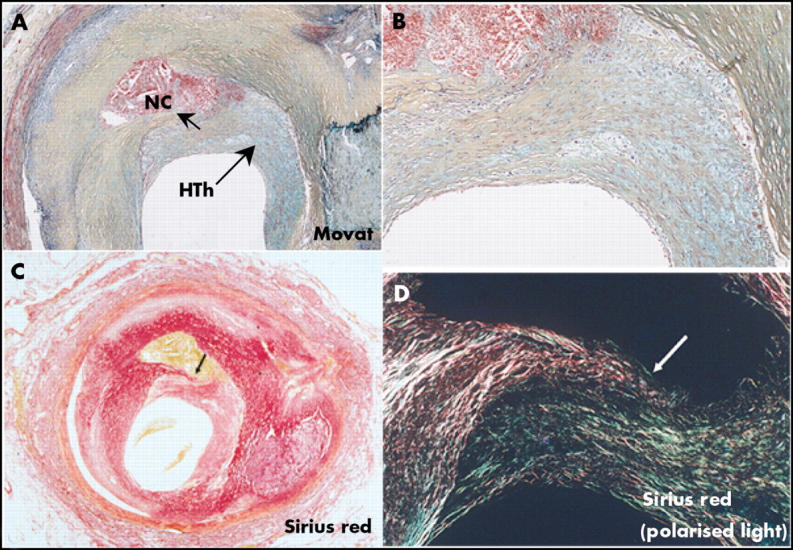
Healed plaque rupture. (A) Areas of intraintimal lipid-rich core with haemorrhage and cholesterol clefts; an old area of necrosis (NC) is seen underlying a healed thrombus (HTh). (B) Higher magnification showing extensive smooth muscle cells (SMCs) within a collagenous proteoglycan-rich neointima (healed thrombus) with clear demarcation from the fibrous region of old plaque to right. (C and D) Layers of collagen by Sirius red staining. (C) Note area of dense, dark red collagen surrounding lipid haemorrhagic cores seen in corresponding view in A. (D) Image taken with polarised light. Dense collagen (type 1) that forms fibrous cap is lighter reddish yellow and is disrupted (arrow), with newer greenish type III collagen on right and above rupture site. (A and B) Movat pentachrome. Reproduced with permission from Burke et al, Circulation 2001;103:934–40.
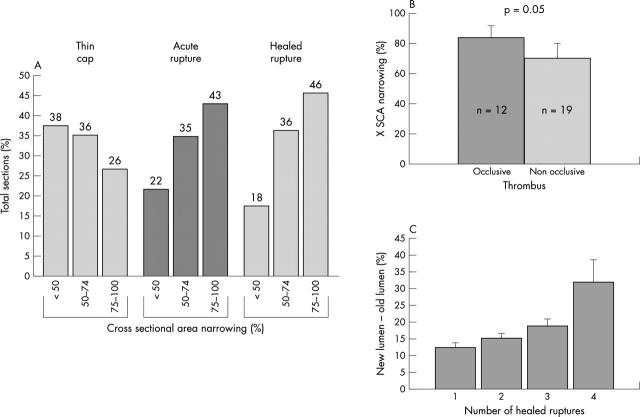
Luminal narrowing as a function of plaque morphology. (A) Severe cross sectional luminal narrowing of > 75% is more common in acute and healed ruptures than in thin cap fibroatheromas (TCFAs). Note 74% of TCFAs showed luminal narrowing ⩽ 74%. (B) Cross sectional luminal narrowing in lesions with occlusive and non-occlusive thrombi; note lesions with occlusive thrombi demonstrate greater luminal stenosis. (C) The change in lumen size is plotted against the number of healed ruptures. While the percentage of stenosis gradually increases with 1–3 underlying healed ruptures, with four previous ruptures, there is a pronounced increase in luminal stenosis. Panel A is reproduced with permission from Virmani R, et al. J Interv Cardiol 2002;15:439–46.
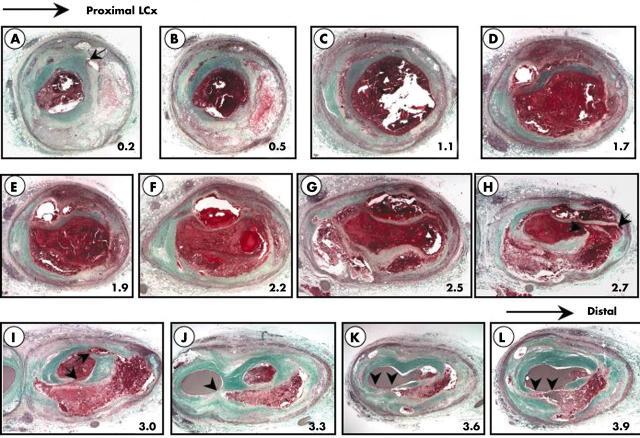
Serial sections of the left circumflex coronary artery from the case shown in fig 2D demonstrating sites of acute and healed plaque rupture and thin cap fibroatheromas (TCFAs) within a relatively short distance. The numbers in the lower right hand corner of the micrographs correspond to the distance in mm from the previous section within a single 5 mm arterial segment. The arrows correspond to rupture sites whether healed or acute while arrowheads represent sites of TCFAs. The first section (A) at 0.2 mm shows a healed plaque rupture; the circumferential repair is rich is proteoglycans (bluish-green). Overall the vessel shows multiple sites of rupture at depths of 2.7 mm and 3.0 mm; an occlusive luminal thrombus is observed in most sections except for panels J–L where the lumen is filled with barium gelatin (greyish material). In the same artery at levels of 3.3 mm, 3.6 mm, and 3.9 mm are multiple TCFAs. Note similar areas of necrosis are found in both deep and superficial locations depending on the level of the section. (Movat pentachrome, ×20).
References
-
- American Heart Association. Heart and stroke statistical update. Dallas, Texas: American Heart Association, 2001.
-
- Burke AP, Farb A, Malcom GT, et al. Coronary risk factors and plaque morphology in men with coronary disease who died suddenly. N Engl J Med 1997;336:1276–82. - PubMed
-
- Burke AP, Farb A, Malcom GT, et al. Effect of risk factors on the mechanism of acute thrombosis and sudden coronary death in women. Circulation 1998;97:2110–6. - PubMed
-
- Virmani R, Kolodgie FD, Burke AP, et al. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–75. - PubMed
-
- Farb A, Burke AP, Tang AL, et al. Coronary plaque erosion without rupture into a lipid core. A frequent cause of coronary thrombosis in sudden coronary death. Circulation 1996;93:1354–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical