

Management and in-hospital outcome of patients with acute myocardial infarction admitted to intensive care units at the turn of the century: results from the French nationwide USIC 2000 registry
- PMID: 15547013
- PMCID: PMC1768566
- DOI: 10.1136/hrt.2003.025460
Management and in-hospital outcome of patients with acute myocardial infarction admitted to intensive care units at the turn of the century: results from the French nationwide USIC 2000 registry
Abstract
Objective: To assess actual practices and in-hospital outcome of patients with acute myocardial infarction on a nationwide scale.
Methods: Of 443 intensive care units in France, 369 (83%) prospectively collected data on all cases of infarction (within < 48 hours of symptom onset) in November 2000.
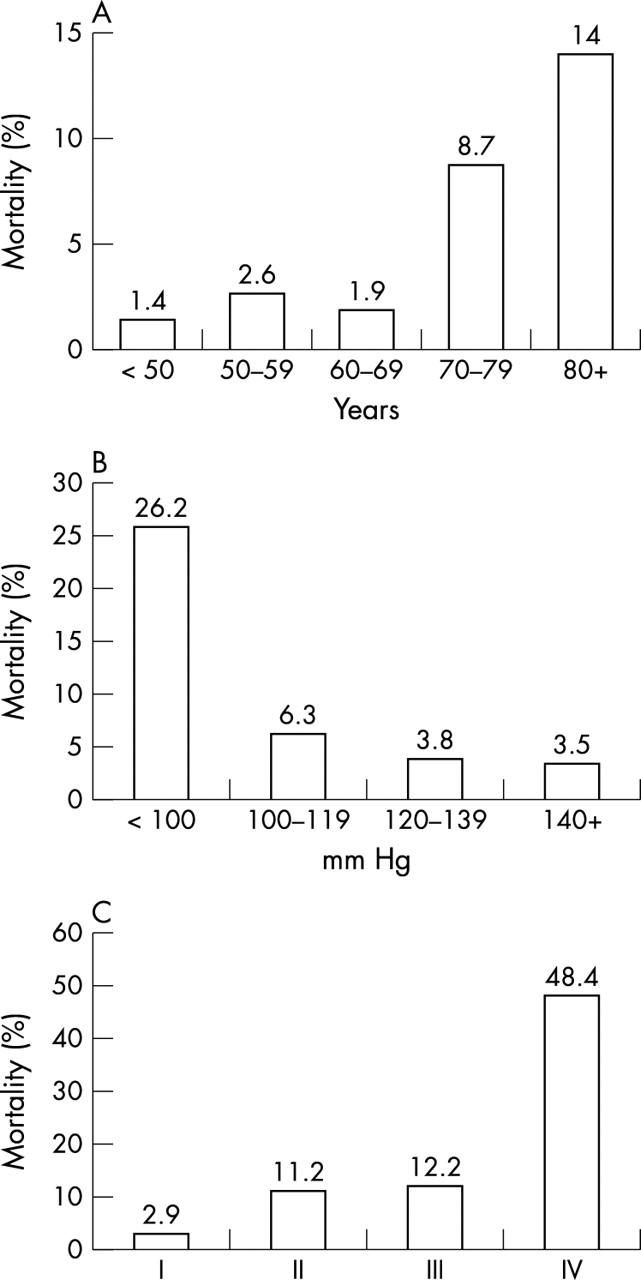
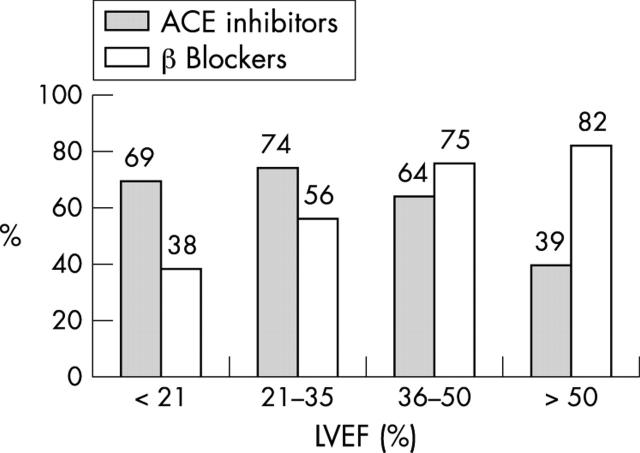
Results: 2320 patients (median age 68 years, 73% men) were included, of whom 83% had ST segment elevation infarction (STEMI). Patients without STEMI were older and had a more frequent history of cardiovascular disease. Median time to admission was 5.0 hours for patients with and 6.5 hours for those without STEMI. Reperfusion therapy was used for 53% of patients with STEMI (thrombolysis 28%, primary angioplasty 25%). In-hospital mortality was 8.7% (5.5% of patients without and 9.3% of those with STEMI). Multivariate analysis found that age, Killip class, lower blood pressure, higher heart rate on admission, anterior location of infarct, STEMI, diabetes mellitus, previous stroke, and no current smoking independently predicted in-hospital mortality. At hospital discharge, 95% received antiplatelet agents, 75% received beta blockers, and over 60% received statins. Angiotensin converting enzyme inhibitors were prescribed for 40% of the patients without and 52% of those with ST elevation.
Conclusions: This nationwide registry, including all types of centres irrespective of their size and experience, shows continued improvement in patient care and outcomes. Time from symptom onset to admission, however, has not improved in recent years and reperfusion therapy is used for just over 50% of patients with STEMI, with an increasing use of primary angioplasty.
Figures
References
-
- Van de Werf F, Ardissino D, Betriu A, et al. The task force on the management of acute myocardial infarction of the European Society of Cardiology. Management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2003;24:28–66. - PubMed
-
- Ryan TJ, Antman EM, Brooks NH, et al. 1999 updated guideline (web version). ACC/AHA guidelines for the management of patients with acute myocardial infarction. A report of the American College of Cardiology/American Heart Association task force on practice guidelines (committee on management of acute myocardial infarction). www.acc.org/clinical/guildelines/nov96/1999/index.htm (accessed 20 Jun 2004).
-
- Hasdai D, Behar S, Wallentin L, et al. A prospective survey of the characteristics, treatments and outcomes of patients with acute coronary syndromes in Europe and the Mediterranean basin: the Euro heart Survey of acute coronary syndromes (Euro heart survey ACS). Eur Heart J 2002;23:1190–201. - PubMed
-
- Marciniak TA, Ellerbeck EF, Radford MJ, et al. Improving the quality of care for Medicare patients with acute myocardial infarction: results from the cooperative cardiovascular project. JAMA 1998;279:1351–7. - PubMed
-
- Berning J, Steenegaard-Hansen F. Early estimation of risk by echocardiographic determination of wall motion index in an unselected population with acute myocardial infarction. Am J Cardiol 1990;65:567–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical