

Women and autoimmune diseases
- PMID: 15550215
- PMCID: PMC3328995
- DOI: 10.3201/eid1011.040367
Women and autoimmune diseases
Abstract
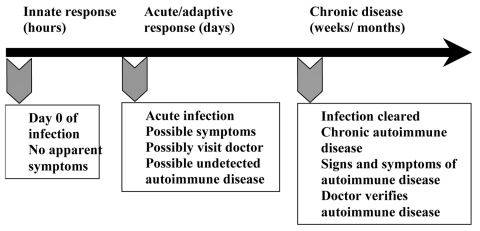
Autoimmune diseases affect approximately 8% of the population, 78% of whom are women. The reasons for the high prevalence in women are unknown, but circumstantial evidence links autoimmune diseases with preceding infections. Animal models of autoimmune diseases have shown that infections can induce autoimmune disease. For example, coxsackievirus B3 (CB3) infection of susceptible mice results in inflammation of the heart (myocarditis) that resembles myocarditis in humans. The same disease can be induced by injecting mice with heart proteins mixed with adjuvant(s), which indicates that an active infection is not necessary for the development of autoimmune disease. We have found that CB3 triggers autoimmune disease in susceptible mice by stimulating elevated levels of proinflammatory cytokines from mast cells during the innate immune response. Sex hormones may further amplify this hyperimmune response to infection in susceptible persons, which leads to an increased prevalence of autoimmune diseases in women.
Figures





Similar articles
-
Mast cells and innate cytokines are associated with susceptibility to autoimmune heart disease following coxsackievirus B3 infection.Autoimmunity. 2004 Mar;37(2):131-45. doi: 10.1080/0891693042000196200. Autoimmunity. 2004. PMID: 15293883
-
Animal models for autoimmune myocarditis and autoimmune thyroiditis.Methods Mol Med. 2004;102:175-93. doi: 10.1385/1-59259-805-6:175. Methods Mol Med. 2004. PMID: 15286386
-
The transition from viral to autoimmune myocarditis.Autoimmunity. 2001;34(3):169-76. doi: 10.3109/08916930109007381. Autoimmunity. 2001. PMID: 11908774 Review.
-
From infection to autoimmunity.J Autoimmun. 2001 May;16(3):175-86. doi: 10.1006/jaut.2000.0492. J Autoimmun. 2001. PMID: 11334481 Review.
-
Viruses as adjuvants for autoimmunity: evidence from Coxsackievirus-induced myocarditis.Rev Med Virol. 2005 Jan-Feb;15(1):17-27. doi: 10.1002/rmv.445. Rev Med Virol. 2005. PMID: 15386590 Review.
Cited by
-
Gender-specific differences in PPARγ regulation of follicular helper T cell responses with estrogen.Sci Rep. 2016 Jun 23;6:28495. doi: 10.1038/srep28495. Sci Rep. 2016. PMID: 27335315 Free PMC article.
-
The PBDE-209 exposure during pregnancy and lactation impairs immune function in rats.Mediators Inflamm. 2012;2012:692467. doi: 10.1155/2012/692467. Epub 2012 Feb 15. Mediators Inflamm. 2012. PMID: 22619485 Free PMC article.
-
Systematic Review and Meta-Analysis of Sex-Specific COVID-19 Clinical Outcomes.Front Med (Lausanne). 2020 Jun 23;7:348. doi: 10.3389/fmed.2020.00348. eCollection 2020. Front Med (Lausanne). 2020. PMID: 32671082 Free PMC article.
-
Tlr7 drives sex- and tissue-dependent effects in Sjögren's disease.Front Cell Dev Biol. 2024 Sep 6;12:1434269. doi: 10.3389/fcell.2024.1434269. eCollection 2024. Front Cell Dev Biol. 2024. PMID: 39310226 Free PMC article.
-
First Insights into the Gut Microbiota of Mexican Patients with Celiac Disease and Non-Celiac Gluten Sensitivity.Nutrients. 2018 Nov 2;10(11):1641. doi: 10.3390/nu10111641. Nutrients. 2018. PMID: 30400238 Free PMC article.
References
-
- National Institutes of Health Autoimmune Disease Coordinating Committee Report. 2002. Bethesda (MD): The Institutes; 2002.
-
- Rose NR. An immunology primer. In: Morton CC, Fagan T, editors. Proceedings from Sex Differences in Immunology and Autoimmunity, Society for Women's Health Research, Boston, MA, 8 Nov 2001. Washington: Society for Women's Health Research; 2002. p. 7–9.
-
- Rose NR. Autoimmune diseases: tracing the shared threads. Hosp Pract. 1997;15:147–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical