

Open port placement of the first laparoscopic port: a safe technique
- PMID: 15554282
- PMCID: PMC3016831
Open port placement of the first laparoscopic port: a safe technique
Abstract
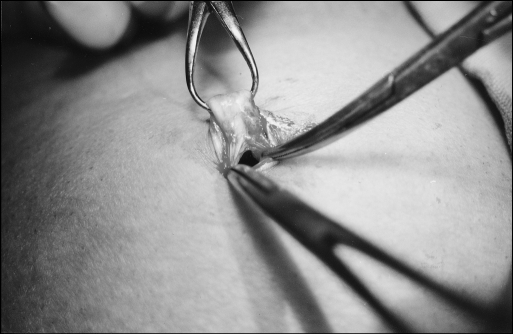
Background: Blind insertion of the Veress needle and of the first trocar is a significant cause of complications in laparoscopic surgery. Despite this risk, the closed technique is still more popular than the open one. Our aim is to report the results of our experience with the routine use of the modified open technique in laparoscopic surgery and to describe the technical details of the creation of pnuemoperitoneum by the open technique that we used.
Methods: A prospective study was conducted in the department of surgery at Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi. A modified method of open laparoscopy was performed on 755 consecutive patients requiring laparoscopy or laparoscopic surgery over a 5-year period from August 1998 to February 2003 in 1 surgical unit.
Results: The mean time taken was 4 minutes (range, 2 to 10). No intraoperative complications occurred during trocar insertion. Forty-nine (6.49%) patients had minor umbilical sepsis, 22 (2.91%) had periumbilical hematoma, but none had umbilical hernia during 3 months of follow-up after surgery.
Conclusion: Based on our own experience, we recommend open laparoscopy as a safe and easy approach for routine laparoscopic interventions.
Figures

Similar articles
-
Laparoscopic Access: Direct Trocar Insertion Versus Open Technique.J Laparoendosc Adv Surg Tech A. 2019 Apr;29(4):489-494. doi: 10.1089/lap.2018.0408. Epub 2019 Jan 10. J Laparoendosc Adv Surg Tech A. 2019. PMID: 30628857 Clinical Trial.
-
Direct trocar insertion technique: an alternative for creation of pneumoperitoneum.JSLS. 2008 Apr-Jun;12(2):156-8. JSLS. 2008. PMID: 18435888 Free PMC article.
-
Routine use of open technique in laparoscopic operations.J Am Coll Surg. 1997 Jan;184(1):58-62. J Am Coll Surg. 1997. PMID: 8989301
-
Laparoscopic entry: a review of techniques, technologies, and complications.J Obstet Gynaecol Can. 2007 May;29(5):433-447. doi: 10.1016/S1701-2163(16)35496-2. J Obstet Gynaecol Can. 2007. PMID: 17493376 Review. English, French.
-
Access techniques: Veress needle--initial blind trocar insertion versus open laparoscopy with the Hasson trocar.Endosc Surg Allied Technol. 1995 Feb;3(1):35-8. Endosc Surg Allied Technol. 1995. PMID: 7757437 Review.
Cited by
-
Open Versus Closed Laparoscopy: Yet an Unresolved Controversy.J Clin Diagn Res. 2016 Feb;10(2):QC04-7. doi: 10.7860/JCDR/2016/18049.7252. Epub 2016 Feb 1. J Clin Diagn Res. 2016. PMID: 27042535 Free PMC article.
-
Surgical Treatment of Recurrent Rectal Prolapse in an Adult Female Black-crested Mangabey (Lophocebus aterrimus) by Colopexy.Comp Med. 2018 Feb 1;68(1):80-83. Comp Med. 2018. PMID: 29460725 Free PMC article.
-
Open laparoscopic access technique: review of 2010 patients.JSLS. 2008 Oct-Dec;12(4):372-5. JSLS. 2008. PMID: 19275851 Free PMC article.
-
A safe quick technique for placement of the first access port for creation of pneumoperitoneum.JSLS. 2011 Oct-Dec;15(4):504-8. doi: 10.4293/108680811X13176785204238. JSLS. 2011. PMID: 22643506 Free PMC article.
-
Veress needle insertion through left lower intercostal space for creating pneumoperitoneum: Experience with 75 cases.J Minim Access Surg. 2012 Jul;8(3):85-9. doi: 10.4103/0972-9941.97590. J Minim Access Surg. 2012. PMID: 22837595 Free PMC article.
References
-
- Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol. 1971;110:886–887 - PubMed
-
- Siren PH, Kurki T. Nationwide analysis of laparoscopic complications. Obstet Gynecol. 1997;89:108–112 - PubMed
-
- Chapron CM, Pierre F, Lacroix S, Querleu D, Lansac J, Dubuisson JB. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg. 1997;185(5):461–465 Comments in: J Am Coll Surg. 1998;186(5):604–605 - PubMed
-
- Geers J, Holden C. Major vascular injuries as a complication of laparoscopic surgery: a report of three cases and review of literature. Am Surg. 1996;62(5):377–379 - PubMed
-
- Champault G, Cazacu F, Taffinder N. Serious trocar accidents in Laparoscopic surgery: A French surgery of 103,852 operations. Surg Laparosc Endosc. 1996;6(5):367–370 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical