

Review
doi: 10.1136/adc.2003.046532.
Interventional cardiac catheterisation in congenital heart disease
Affiliations
- PMID: 15557059
- PMCID: PMC1719759
- DOI: 10.1136/adc.2003.046532
Item in Clipboard
Review
Interventional cardiac catheterisation in congenital heart disease
Arch Dis Child.
2004 Dec.
Abstract
As a result of recent technological advances, more types of congenital heart disease are amenable to treatment in the cardiac catheter laboratory than ever before.1 Improved imaging techniques allow for better selection of patients, and the development of a wide range of devices specifically for use in children means that many patients can avoid surgery altogether, while those with complex congenital heart disease may require fewer or less complex surgical procedures.2 This allows for a quicker recovery and a shorter hospital stay, and gives many patients an improved quality of life in the short to medium term. However, the long term outcome for many of the newer forms of intervention is still unknown.
Figures
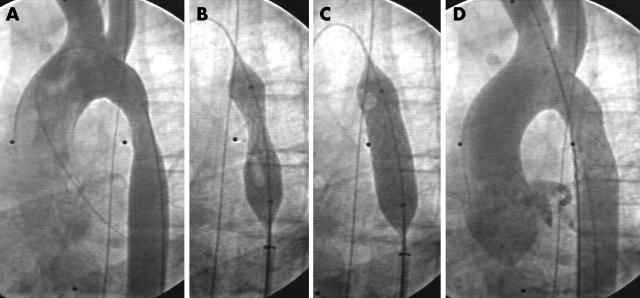
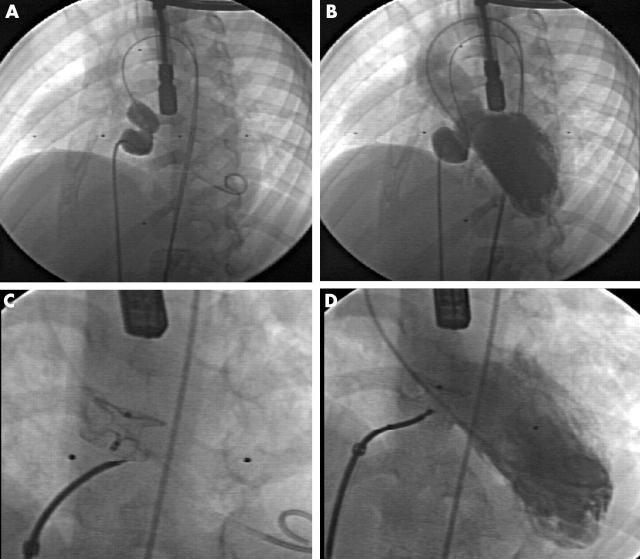
Angiographic pictures of stent insertion for re-coarctation following subclavian flap repair; (A) pre-procedure, (B) stent insertion, (C) stent expansion by inflation of internal balloon, (D) final result.
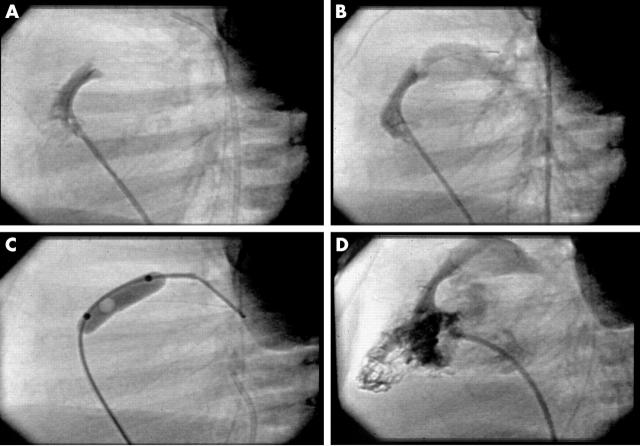
Angiographic pictures of radiofrequency perforation for pulmonary atresia; (A) catheter against imperforate valve (lateral projection), (B) radiofrequency wire across valve, (C) balloon dilation of valve perforation, (D) antegrade flow established.

Devices for duct occlusion: a pair of Amplatzer Ductocclude devices, and a pair of Cook MReye coils.
An Amplatzer Septal Occluder for closure of atrial septal defects.
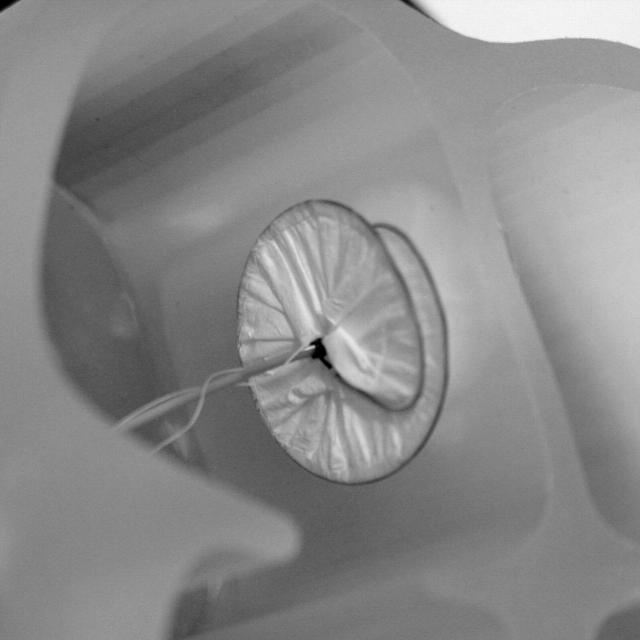
A Helex device for closure of atrial septal defects.
Angiographic pictures of device occlusion of a VSD; (A) + (B) balloon sizing of the defect, (C) + (D) deployment of the device.
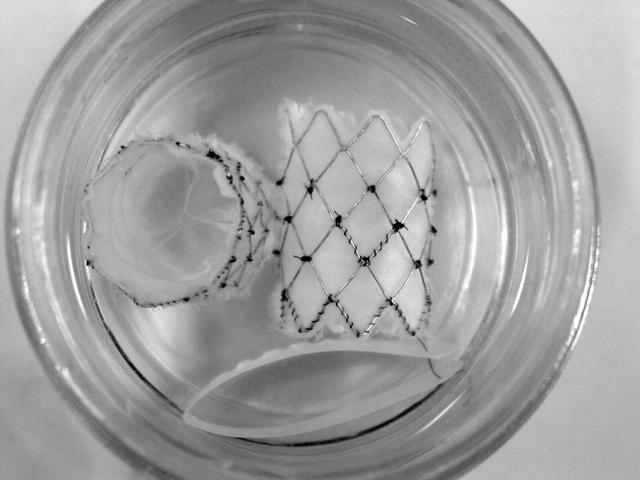
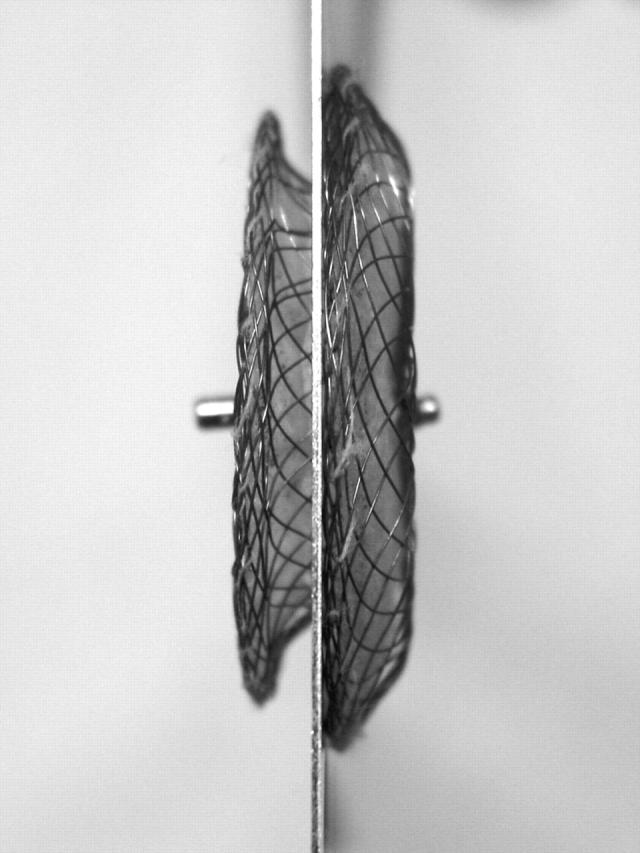
A pair of implantable pulmonary valved stents. The fine tissue of a closed valve is shown in the device on the left.
Similar articles
-
Therapeutic cardiac catheterization for congenital heart disease--a new era in pediatric care.J Pediatr Nurs. 2001 Oct;16(5):300-7. doi: 10.1053/jpdn.2001.26567. J Pediatr Nurs. 2001. PMID: 11598862
-
[Options for interventional heart catheterization in congenital heart disease].Ther Umsch. 2001 Feb;58(2):99-104. doi: 10.1024/0040-5930.58.2.99. Ther Umsch. 2001. PMID: 11234458 Review. German.
-
Interventional catheterization in paediatric cardiology.Eur Heart J. 1995 Dec;16(12):1767-72. doi: 10.1093/oxfordjournals.eurheartj.a060826. Eur Heart J. 1995. PMID: 8682005 Review.
-
Paediatric cardiac catheterization: innovations.Can J Anaesth. 1995 Apr;42(4):310-29. doi: 10.1007/BF03010708. Can J Anaesth. 1995. PMID: 7788828 Review.
-
Versatility of the microvena snare in pediatric interventional cardiac catheterization.Cathet Cardiovasc Diagn. 1996 Apr;37(4):456-8. doi: 10.1002/(SICI)1097-0304(199604)37:4<456::AID-CCD19>3.0.CO;2-D. Cathet Cardiovasc Diagn. 1996. PMID: 8721706
Cited by
-
[Catheter interventions for congenital heart disease].Herz. 2008 Dec;33(8):592-600. doi: 10.1007/s00059-008-3133-1. Epub 2009 Jan 8. Herz. 2008. PMID: 19137250 Review. German.
-
Real-time automatic image-based slice tracking of gadolinium-filled balloon wedge catheter during MR-guided cardiac catheterization: A proof-of-concept study.Magn Reson Med. 2024 Jan;91(1):388-397. doi: 10.1002/mrm.29822. Epub 2023 Sep 7. Magn Reson Med. 2024. PMID: 37676923 Free PMC article.
-
Congenital Heart Disease in Low- and Lower-Middle-Income Countries: Current Status and New Opportunities.Curr Cardiol Rep. 2019 Nov 29;21(12):163. doi: 10.1007/s11886-019-1248-z. Curr Cardiol Rep. 2019. PMID: 31784844 Review.
-
Perioperative care of neonates with critical pulmonary stenosis: Case report.Medicine (Baltimore). 2024 Feb 23;103(8):e37203. doi: 10.1097/MD.0000000000037203. Medicine (Baltimore). 2024. PMID: 38394548 Free PMC article.
-
The causes of Charcot-Marie-Tooth disease.Cell Mol Life Sci. 2003 Dec;60(12):2547-60. doi: 10.1007/s00018-003-3133-5. Cell Mol Life Sci. 2003. PMID: 14685682 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials