

Congenital anomaly surveillance in England--ascertainment deficiencies in the national system
- PMID: 15561730
- PMCID: PMC539849
- DOI: 10.1136/bmj.38300.665301.3A
Congenital anomaly surveillance in England--ascertainment deficiencies in the national system
Abstract
Objective: Firstly, to assess the completeness of ascertainment in the National Congenital Anomaly System (NCAS), the basis for congenital anomaly surveillance in England and Wales, and its variation by defect, geographical area, and socioeconomic deprivation. Secondly, to assess the impact of the lack of data on pregnancies terminated because of fetal anomaly.
Design: Comparison of the NCAS with four local congenital anomaly registers in England.
Setting: Four regions in England covering some 109,000 annual births.
Participants: Cases of congenital anomalies registered in the NCAS (live births and stillbirths) and independently registered in the four local registers (live births, stillbirths, fetal losses from 20 weeks' gestation, and pregnancies terminated after prenatal diagnosis of fetal anomaly).
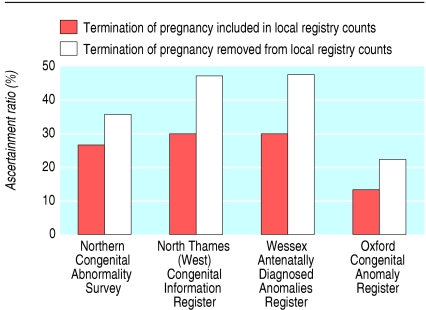
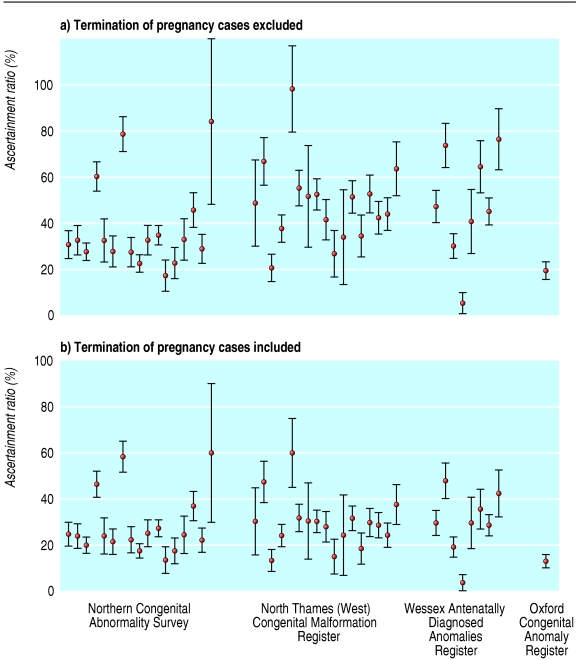
Main outcome measure: The ratio of cases identified by the national register to those in local registry files, calculated for different specified anomalies, for whole registry areas, and for hospital catchment areas within registry boundaries.
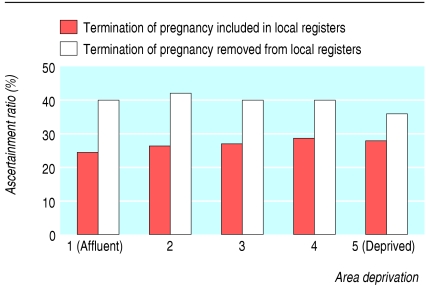
Results: Ascertainment by the NCAS (compared with data from local registers, from which terminations of pregnancy were removed) was 40% (34% for chromosomal anomalies and 42% for non-chromosomal anomalies) and varied markedly by defect, by local register, and by hospital catchment area, but not by area deprivation. When terminations of pregnancy were included in the register data, ascertainment by NCAS was 27% (19% for chromosomal anomalies and 31% for non-chromosomal anomalies), and the geographical variation was of a similar magnitude.
Conclusion: The surveillance of congenital anomalies in England is currently inadequate because ascertainment to the national register is low and non-uniform and because no data exist on termination of pregnancy resulting from prenatal diagnosis of fetal anomaly.
Figures
References
-
- Macfarlaine A, Mugford M. Birthcounts. Statistics of pregnancy and childbirth. London Stationery Office, 2000.
-
- Congenital malformations statistical notifications 1994. London: Stationery Office, 1997. (Series MB3, No 10.)
-
- Payne JN. Limitations of the OPCS congenital malformation notification systems illustrated by examination of congenital malformations of the cardiovascular systems in districts within the Trent region. Public Health 1992;106: 437-48. - PubMed
-
- Office for Population Censuses and Surveys. The OPCS monitoring scheme for congenital malformations occasional paper 43. A review by a working group of the registrar general's medical advisory committee. London: OPCS, 1995.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical