

Maternal blood pressure in pregnancy, birth weight, and perinatal mortality in first births: prospective study
- PMID: 15561733
- PMCID: PMC534837
- DOI: 10.1136/bmj.38258.566262.7C
Maternal blood pressure in pregnancy, birth weight, and perinatal mortality in first births: prospective study
Abstract
Objective: To investigate the relation of diastolic blood pressure in pregnancy with birth weight and perinatal mortality.
Design: Prospective study.
Setting: 15 maternity units in one London health region, 1988-2000.
Participants: 210 814 first singleton births of babies weighing more than 200 g among mothers with no hypertension before 20 weeks' gestation and without proteinuria, delivering between 24 and 43 weeks' gestation.
Main outcome measures: Birth weight and perinatal mortality.
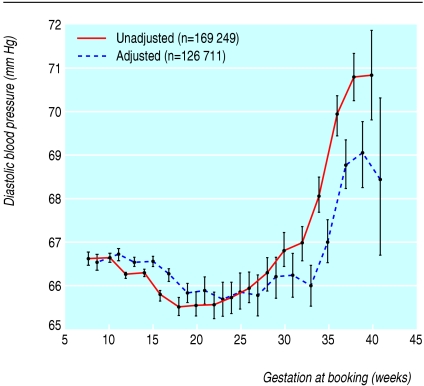
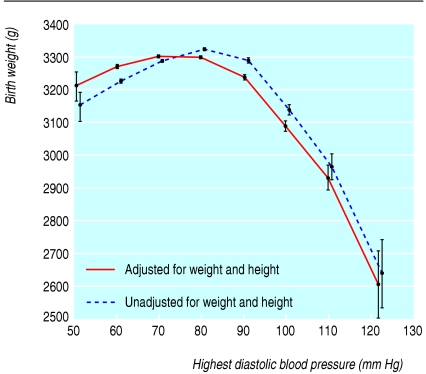
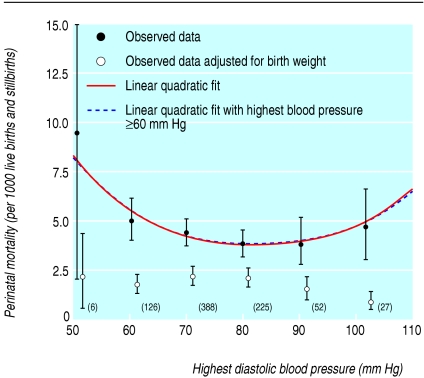
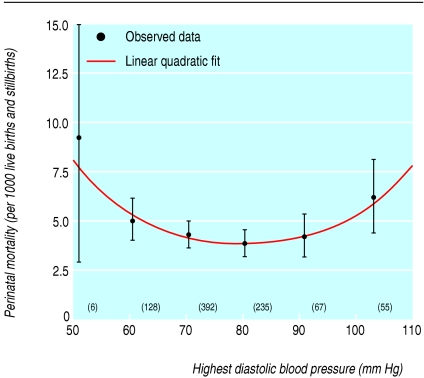
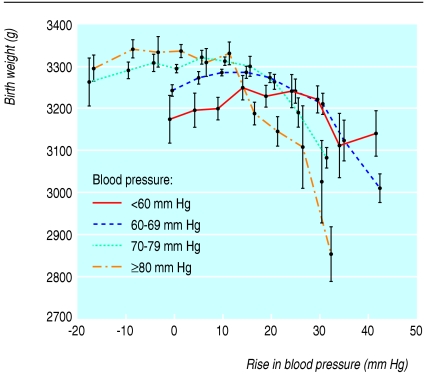
Results: The mean (SD) birth weight of babies born to mothers with no hypertension before 20 weeks' gestation or proteinuria was 3282 g (545 g) and there were 1335 perinatal deaths, compared with 94 perinatal deaths among women with proteinuria or a history of hypertension. Diastolic blood pressure at booking for antenatal checks was progressively higher from weeks 34 to 40 of gestation. The birth weight of babies being delivered after 34 weeks was highest for highest recorded maternal diastolic blood pressures of between 70 and 80 mm Hg and lower for blood pressures outside this range. Both low and high diastolic blood pressures were associated with statistically significantly higher perinatal mortality. Using a linear quadratic model, 94 of 825 (11.4%) perinatal deaths could be attributed to mothers having blood pressure differing from the optimal blood pressure (82.7 mm Hg) predicted by the fitted model. Most of these excess deaths occurred with blood pressures below the optimal value.
Conclusions: Both low and high diastolic blood pressures in women during pregnancy are associated with small babies and high perinatal mortality.
Figures
References
-
- American College of Obstetricians and Gynecologists. Hypertension in pregnancy. ACOG, 1996.
-
- Anon. Report on confidential enquiries into maternal deaths in the United Kingdom 1994-1996. London: Stationery Office, 1998.
-
- Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2004;360: 1903-13. - PubMed
-
- Rowe PC. Orthostatic intolerance and chronic fatigue syndrome: new light on an old problem. J Pediatr 2002;140: 387-9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical