

Use of a computerized guideline for glucose regulation in the intensive care unit improved both guideline adherence and glucose regulation
- PMID: 15561795
- PMCID: PMC551549
- DOI: 10.1197/jamia.M1598
Use of a computerized guideline for glucose regulation in the intensive care unit improved both guideline adherence and glucose regulation
Abstract
Objective: To measure the impact of a computerized guideline for glucose regulation in an ICU.
Design: A randomized, controlled trial with an off-on-off design.
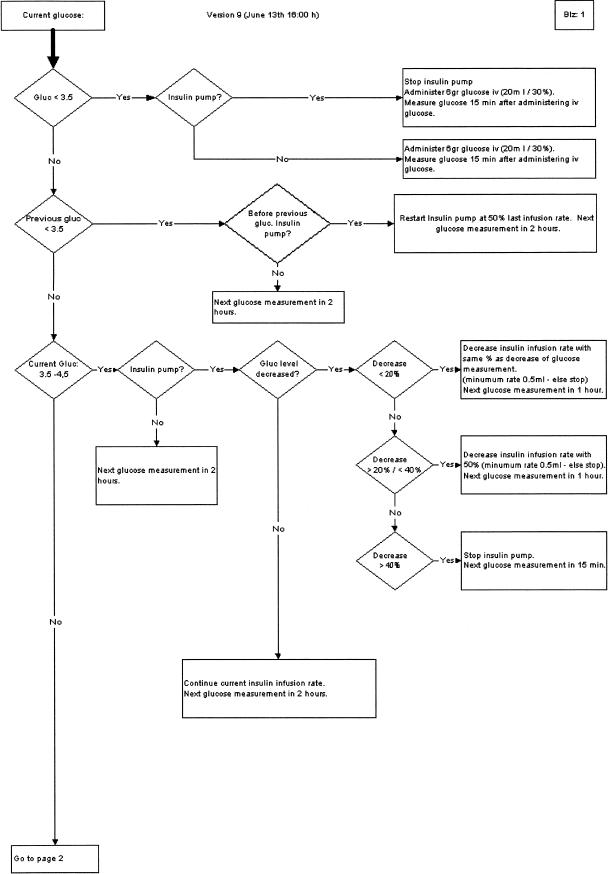
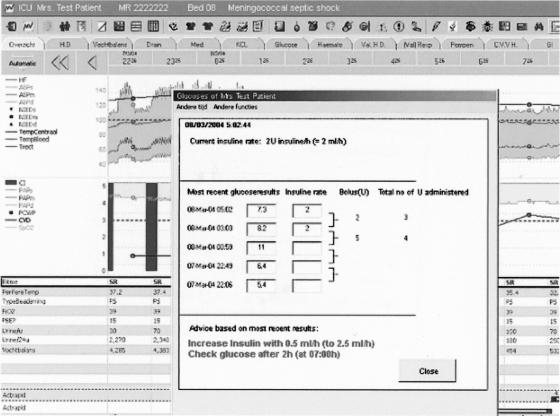
Methods: We implemented a glucose regulation guideline in an intensive care unit in paper form during the first study period. During the second period, the guideline was randomly applied in either paper or computerized form. In the third period, the guideline was available only in paper form.
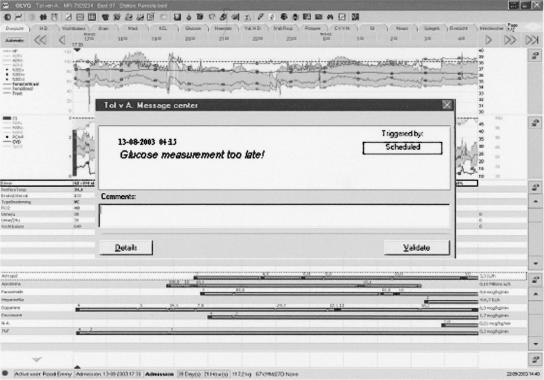
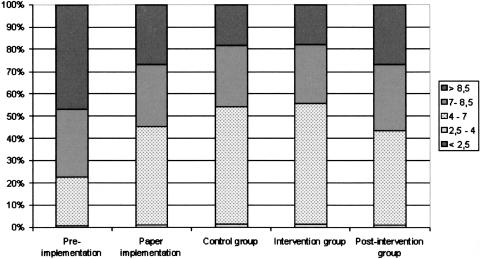
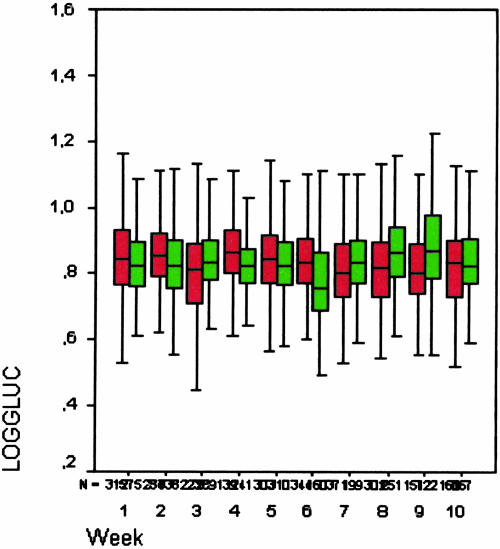
Measurements and results: We analyzed data for 484 patients. During the intervention period, the control group included 54 patients and the computerized intervention group included 66 patients. The two guideline-related outcome measures consisted of compliance with: (a) glucose measurement timing recommendations and (b) insulin dose advice. We measured clinical impact as the proportion of time that glucose levels fell within target range. In the first (paper-based) study period, 29.0% of samples occurred with optimal timing; during the second period, this increased to 35.5% for paper-based and to 40.2% for computerized protocols. The third study period timeliness scores reverted to the first period rates. Late (suboptimal) sampling occurred for 66% of glucose measurements in the first study period, for 42% of paper-based and 28% of computer-based protocol samples in the second period, and for 50.0% of samples in the third study period. In the first study period, insulin-dosing guideline compliance was 56.3%; in the second period, it was 64.2% for paper-based and 77.3% for computer-based protocols, and it fell to 42.4% in the third period. For the second study period, the time that a patient's glucose values fell within target range improved for both the control (52.9%) and the computerized groups (54.2%) compared with the first study period (44.3%) and the third period (42.3%).
Conclusion: Implementing a computerized version of a guideline significantly improved timeliness of measurements and glucose level regulation for critically ill patients compared with implementing a paper-based version of the guideline.
Figures
References
-
- Mizock BA. Alterations in fuel metabolism in critical illness: hyperglycaemia. Best Pract Res Clin Endocrinol Metab. 2001;15:533–51. - PubMed
-
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin treatment in critically ill patients. N Engl J Med. 2001;345:1359–67. - PubMed
-
- Preiser JC, Devos P, Van den Berghe G. Tight control of glycaemia in critically ill patients. Curr Opin Clin Nutr Metab Care. 2002;5:533–7. - PubMed
-
- Capes S, Hunt D, Malmberg K, Gerstein H. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic review. Lancet. 2000;355:773–8. - PubMed
-
- Bolk J, Van der Ploeg T, Cornel JH, Arnold AD, Sepers J, Umans VA. Impaired glucose metabolism predicts mortality after a myocardial infarction. Int J Cardiol. 2001;79:207–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
