

National surveillance of antimicrobial resistance in Pseudomonas aeruginosa isolates obtained from intensive care unit patients from 1993 to 2002
- PMID: 15561832
- PMCID: PMC529178
- DOI: 10.1128/AAC.48.12.4606-4610.2004
National surveillance of antimicrobial resistance in Pseudomonas aeruginosa isolates obtained from intensive care unit patients from 1993 to 2002
Abstract
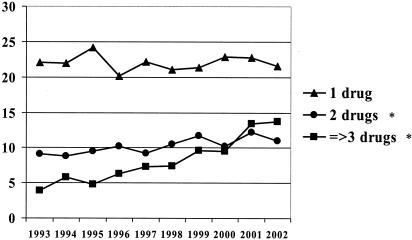
Nosocomial infections caused by Pseudomonas aeruginosa in critically ill patients are often difficult to treat due to resistance to multiple antimicrobials. The purpose of this study was to evaluate antimicrobial resistance among P. aeruginosa isolates from intensive care unit patients in the United States from 1993 to 2002 by using the Intensive Care Unit Surveillance Study database. Over the 10-year period, susceptibility of 13,999 nonduplicate isolates of P. aeruginosa was analyzed. From 1993 to 2002, nationwide increases in antimicrobial resistance were greatest for ciprofloxacin, imipenem, tobramycin, and aztreonam. Rates of multidrug resistance (resistance to > or =3 of the following drugs: ceftazidime, ciprofloxacin, tobramycin, and imipenem) increased from 4% in 1993 to 14% in 2002. The lowest dual resistance rates were observed between aminoglycosides or fluoroquinolones with piperacillin-tazobactam while the highest were for those that included beta-lactams and ciprofloxacin. Ongoing surveillance studies are crucial in monitoring antimicrobial susceptibility patterns and selecting empirical treatment regimens.
Figures
References
-
- Alverez-Lerma, F., et al. 1996. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. Intensive Care Med. 22:387-394. - PubMed
-
- Flamm, R. K., M. K. Weaver, C. Thornsberry, M. E. Jones, J. A. Karlowsky, and D. F. Sahm. 2004. Factors associated with relative rates of antibiotic resistance in Pseudomonas aeruginosa isolates tested in clinical laboratories in the United States from 1999 to 2002. Antimicrob. Agents Chemother. 48:2431-2436. - PMC - PubMed
-
- Gales, A. C., R. N. Jones, J. Turnidge, R. Rennie, and R. Ramphal. 2001. Characterization of Pseudomonas aeruginosa isolates: occurrence rates, antimicrobial susceptibility patterns, and molecular typing in the global SENTRY Antimicrobial Surveillance Program, 1997-1999. Clin. Infect. Dis. 32:S146-S155. - PubMed
-
- Haley, R. W., D. H. Culver, J. W. White, W. M. Morgan, T. G. Emori, V. P. Munn, and T. M. Hooton. 1985. The efficacy of infection surveillance and control programs in preventing nosocomial infections in US hospitals. Am. J. Epidemiol. 121:182-205. - PubMed
-
- Hanberger, H., J. A. Garcia-Rodriguez, M. Gobernado, et al. 1999. Antibiotic susceptibility among aerobic gram-negative bacilli in intensive care units in 5 European countries. JAMA 281:67-71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
