

Transmyocardial laser revascularization as an adjunct to coronary artery bypass grafting: a randomized, multicenter study with 4-year follow-up
- PMID: 15562842
- PMCID: PMC521762
Transmyocardial laser revascularization as an adjunct to coronary artery bypass grafting: a randomized, multicenter study with 4-year follow-up
Abstract
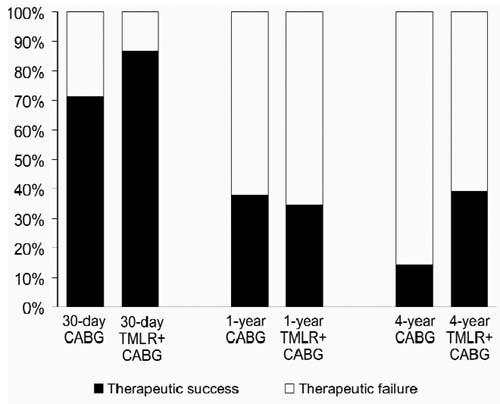
We evaluated transmyocardial laser revascularization (TMLR) with coronary artery bypass grafting (CABG) versus CABG alone for severe coronary artery disease involving 21 myocardial region unsuited for CABG. At 4 centers, 44 consecutive patients were randomized for CABG+TMLR (n = 23) or CABG alone (n = 21). Operative and in-hospital mortality and morbidity rates were monitored. Clinical status was evaluated at hospital discharge, 1 year, and 4 years. Success was characterized by relief of angina and freedom from repeat revascularization and death. Preoperatively, 20 patients (47%) were at high risk. The CABG technique, number of grafts, and target vessels were similar in both groups. Patients undergoing CABG+TMLR received 25 +/- 11 laser channels. Their < or = 30-day mortality was 13% (3/23) compared with 28% (6/21) after CABG alone (P = 0.21). There were no significant intergroup differences in the number of intraoperative or in-hospital adverse events. The follow-up period was 50.3 +/- 17.8 months for CABG alone and 48.1 +/- 16.8 months for CABG+TMLR. Both groups had substantially improved angina and functional status at 1 and 4 years, with no significant differences in cumulative 4-year mortality. The incidence of repeat revascularization was 24% after CABG alone versus none after CABG+TMLR (P < 0.05). The 4-year event-free survival rate was 14% versus 39%, respectively (P < 0.064). In conclusion, CABG+TMLR appears safe and poses no additional threat for high-risk patients. Improved overall success and repeat revascularization rates may be due to better perfusion of ischemic areas not amenable to bypass. Further studies are warranted to determine whether these trends are indeed significant.
References
-
- Higgins TL, Estafanous FG, Loop FD, Beck GJ, Blum JM, Paranandi L. Stratification of morbidity and mortality outcome by preoperative risk factors in coronary artery bypass patients. A clinical severity score [published erratum appears in JAMA 1992;268:1860]. JAMA 1992;267:2344–8. - PubMed
-
- Bell MR, Gersh BJ, Schaff HV, Holmes DR Jr, Fisher LD, Alderman EL, et al. Effect of completeness of revascularization on long-term outcome of patients with three-vessel disease undergoing coronary artery bypass surgery. A report from the Coronary Artery Surgery Study (CASS) Registry. Circulation 1992;86:446–57. - PubMed
-
- Jones EL, Craver JM, Guyton RA, Bone DK, Hatcher CR Jr, Riechwald N. Importance of complete revascularization in performance of the coronary bypass operation. Am J Cardiol 1983;51:7–12. - PubMed
-
- Jones EL, Weintraub WS. The importance of completeness of revascularization during long-term follow-up after coronary artery operations. J Thorac Cardiovasc Surg 1996;112: 227–37. - PubMed
-
- Horvath KA, Cohn LH, Cooley DA, Crew JR, Frazier OH, Griffith BP, et al. Transmyocardial laser revascularization: results of a multicenter trial with transmyocardial laser revascularization used as sole therapy for end-stage coronary artery disease. J Thorac Cardiovasc Surg 1997;113:645–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical