

Composite graft endocarditis: repair with a mechanical prosthesis
- PMID: 15562854
- PMCID: PMC521777
Composite graft endocarditis: repair with a mechanical prosthesis
Abstract
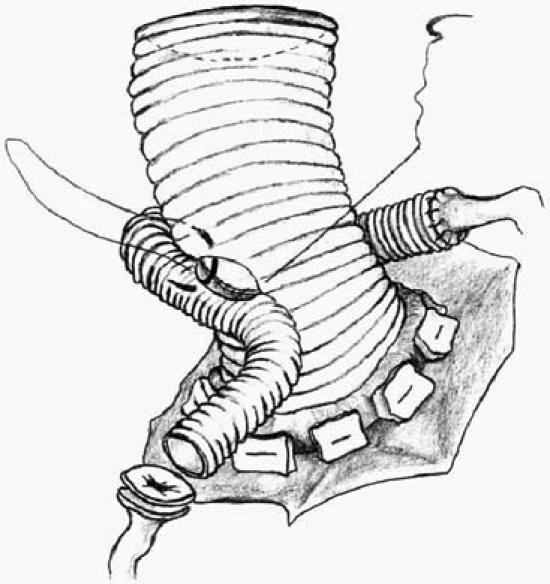
We report the case of a 64-year-old man who developed a mediastinal pseudoaneurysm due to severe endocarditis, 2 years after aortic root replacement with a prosthetic composite graft containing a mechanical valve. After a short period of stabilization and antibiotic therapy, the patient underwent surgery. The coronary buttons and the sewing ring of the composite graft were found to be detached from the graft and the annulus, respectively. Re-replacement with a prosthetic composite graft (Dacron graft with a mechanical valve) by the Cabrol procedure was performed. Although the homograft is considered by many surgeons to be the best graft for aortic root replacement, the synthetic composite graft can also be used to treat composite graft endocarditis successfully. The technical aspects of homograft versus synthetic aortic root replacement in patients with endocarditis are discussed briefly.
Figures


Similar articles
-
Homograft subclavian interposition graft to left main coronary artery ostium in aortic root replacement.Eur J Cardiothorac Surg. 2016 Jan;49(1):350-1. doi: 10.1093/ejcts/ezv046. Epub 2015 Feb 10. Eur J Cardiothorac Surg. 2016. PMID: 25669643
-
[Surgical treatment with the freestyle bioprosthesis and omentopexy for prosthetic valve endocarditis after aortic root replacement].Kyobu Geka. 2006 Jul;59(7):531-5. Kyobu Geka. 2006. PMID: 16856526 Japanese.
-
Aortic root replacement with a mechanical valve and prosthetic conduit for the complicated degeneration of the ascending aorta resulting from infective endocarditis.Ann Thorac Cardiovasc Surg. 2007 Oct;13(5):355-9. Ann Thorac Cardiovasc Surg. 2007. PMID: 17954997
-
The impact of aortic valve homografts on the treatment of aortic prosthetic valve endocarditis.Semin Thorac Cardiovasc Surg. 1995 Jan;7(1):25-31. Semin Thorac Cardiovasc Surg. 1995. PMID: 7893834 Review.
-
Management of thoracic aortic graft infections.J Card Surg. 2018 Oct;33(10):658-665. doi: 10.1111/jocs.13792. Epub 2018 Sep 3. J Card Surg. 2018. PMID: 30178475 Review.
Cited by
-
Case Report of an Infrequent Complication of Infective Endocarditis: The Complete Detachment from the Aorta of the Previous Vein Graft Anastomosis.Aorta (Stamford). 2018 Dec;6(6):139-141. doi: 10.1055/s-0039-1678554. Epub 2019 Apr 24. Aorta (Stamford). 2018. PMID: 31018237 Free PMC article.
References
-
- Niwaya K, Knott-Craig CJ, Santangelo K, Lane MM, Chandrasekeran K, Elkins RC. Advantage of autograft and homograft valve replacement for complex aortic valve endocarditis. Ann Thorac Surg 1999;67:1603–8. - PubMed
-
- Haydock D, Barratt-Boyes B, Macedo T, Kirklin JW, Blackstone E. Aortic valve replacement for active infectious endocarditis in 108 patients. A comparison of freehand allograft valves with mechanical prostheses and bioprostheses. J Thorac Cardiovasc Surg 1992;103:130–9. - PubMed
-
- Lytle BW, Sabik JF, Blackstone EH, Svensson LG, Pettersson GB, Cosgrove DM 3rd. Reoperative cryopreserved root and ascending aorta replacement for acute aortic prosthetic valve endocarditis. Ann Thorac Surg 2002;74:S1754–7; S1792–9. - PubMed
-
- Aagaard J, Andersen PV. Acute endocarditis treated with radical debridement and implantation of mechanical or stented bioprosthetic devices. Ann Thorac Surg 2001;71: 100–4. - PubMed
-
- Bauernschmitt R, Jakob HG, Vahl CF, Lange R, Hagl S. Operation for infective endocarditis: results after implantation of mechanical valves. Ann Thorac Surg 1998;65:359–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical