

How doctors discuss major interventions with high risk patients: an observational study
- PMID: 15564228
- PMCID: PMC544994
- DOI: 10.1136/bmj.38293.435069.DE
How doctors discuss major interventions with high risk patients: an observational study
Abstract
Objective: To investigate the difficulties doctors face in discussing treatment options with patients with acute, life threatening illness and major comorbidities.
Design: Observational study of doctor-patient interviews based on a standardised clinical scenario involving high risk surgery in a hypothetical patient (played by an actor) with serious comorbidities.
Participants: 30 trainee doctors 3-5 years after graduation.
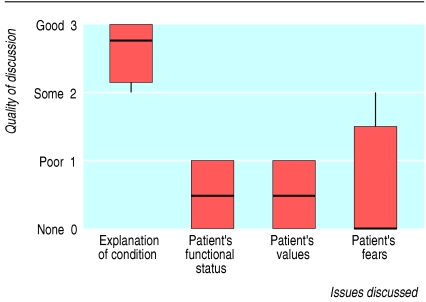
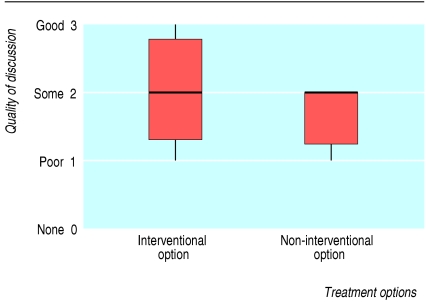
Main outcome measures: Adequacy of coverage of various aspects was scored from 3 (good) to 0 (not discussed).
Results: The medical situation was considered to be well described (median score 2.7 (interquartile range 2.1-3.0)), whereas the patient's functional status, values, and fears were poorly or minimally addressed (scores 0.5 (0.0-1.0), 0.5 (0.0-1.0), and 0.0 (0.0-1.5), respectively; all P < 0.001 v score for describing the medical situation). Twenty nine of the doctors indicated that they wished to include the patient's family in the discussion, but none identified a preferred surrogate decision maker. Six doctors suggested that the patient alone should speak with his family to reach a decision without the doctor being present. The doctors were reluctant to give advice, despite it being directly requested: two doctors stated that a doctor could not give advice, while 17 simply restated the medical risks, without advocating any particular course. Of the 11 who did offer advice, eight advocated intervention.
Conclusions: Doctors focused on technical medical issues and placed much less emphasis on patient issues such as functional status, values, wishes, and fears. This limits doctors' ability to offer suitable advice about treatment options. Doctors need to improve their communication skills in this difficult but common clinical situation.
Figures
References
-
- Schwartz CE, Goulet JL, Gorski V, Selwyn PA. Medical residents' perceptions of end-of-life care training in a large urban teaching hospital. J Palliat Med 2003;6: 37-44. - PubMed
-
- Thistlethwaite JE. Developing an OSCE station to assess the ability of medical students to share information and decisions with patients: issues relating to inter-rater reliability and use of simulated patients. Educ Health (Abingdon) 2002;15: 170-9. - PubMed
-
- Pochard F, Grassin M, Kentish-Barnes N, Azoulay E. Patient autonomy and the end of life. Crit Care Med 2003;31: 662-3. - PubMed
-
- Schneider C. The practice of autonomy, patients, doctors and medical decisions. Oxford: Oxford University Press, 1998.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical