

Interactions between GABAergic and cholinergic processes in the nucleus pontis oralis: neuronal mechanisms controlling active (rapid eye movement) sleep and wakefulness
- PMID: 15564583
- PMCID: PMC6730134
- DOI: 10.1523/JNEUROSCI.1987-04.2004
Interactions between GABAergic and cholinergic processes in the nucleus pontis oralis: neuronal mechanisms controlling active (rapid eye movement) sleep and wakefulness
Abstract
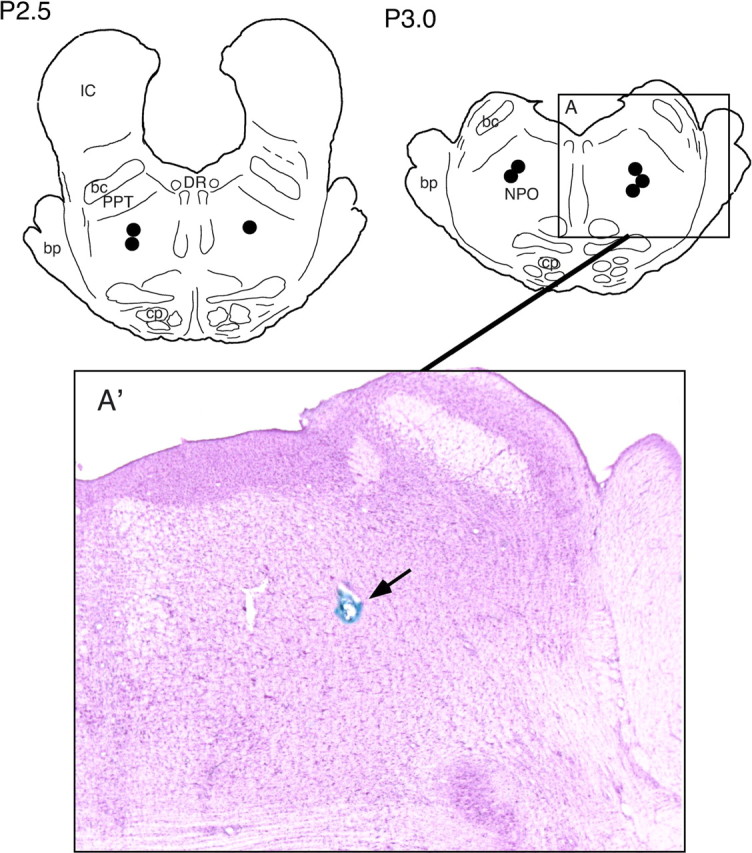
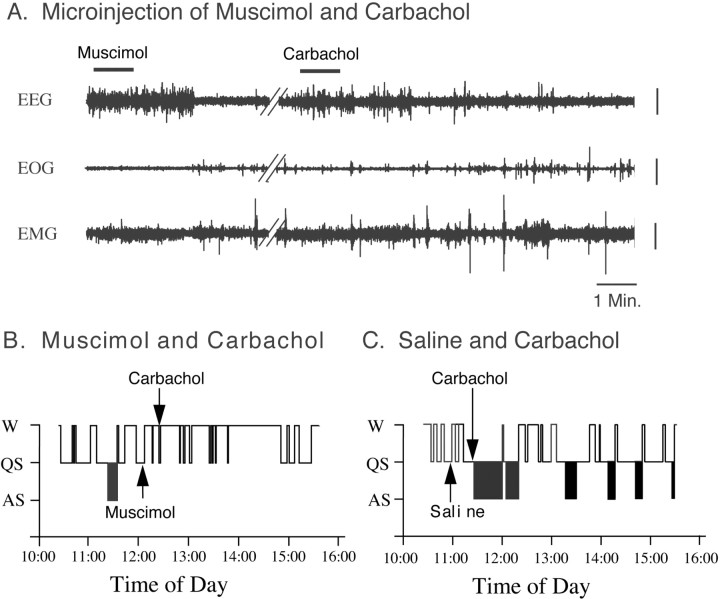
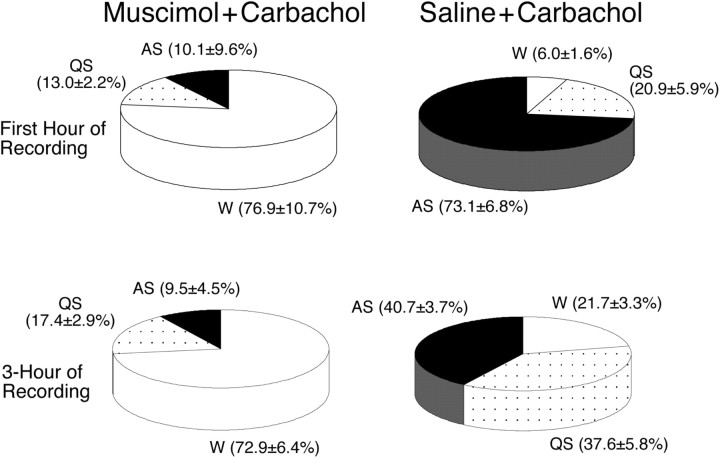
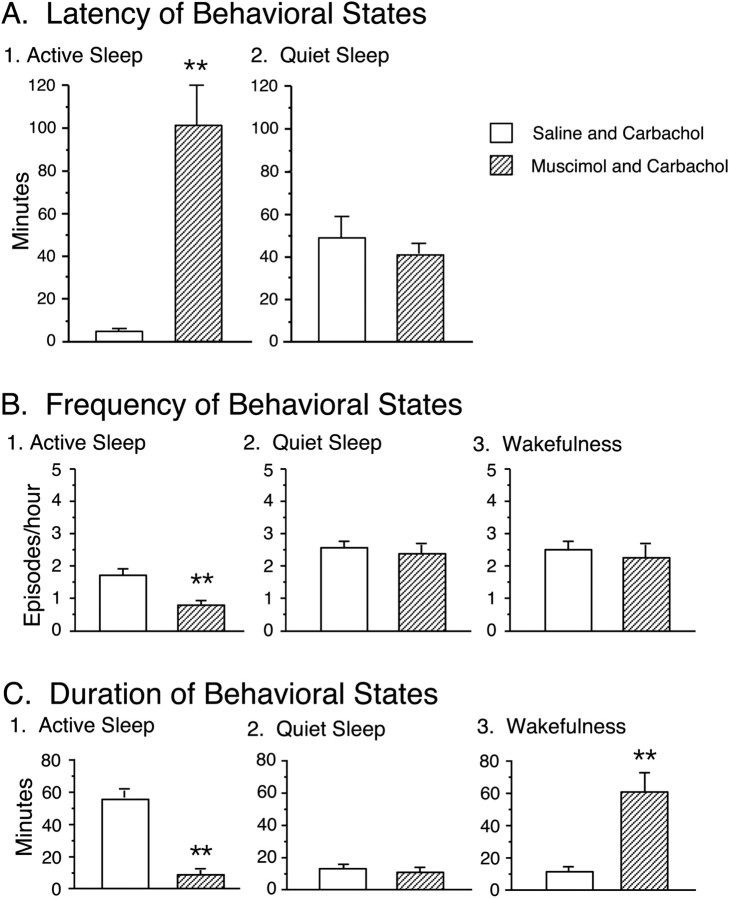
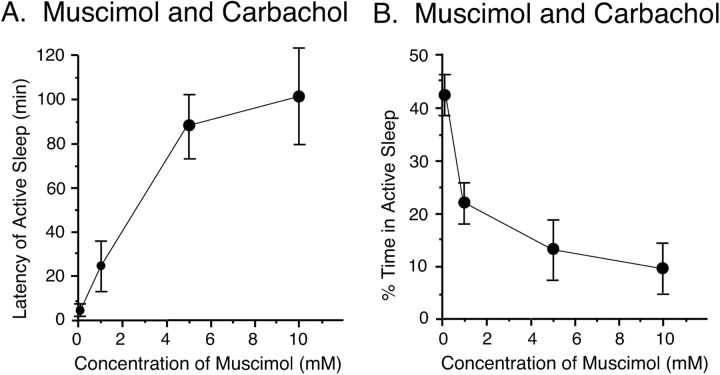
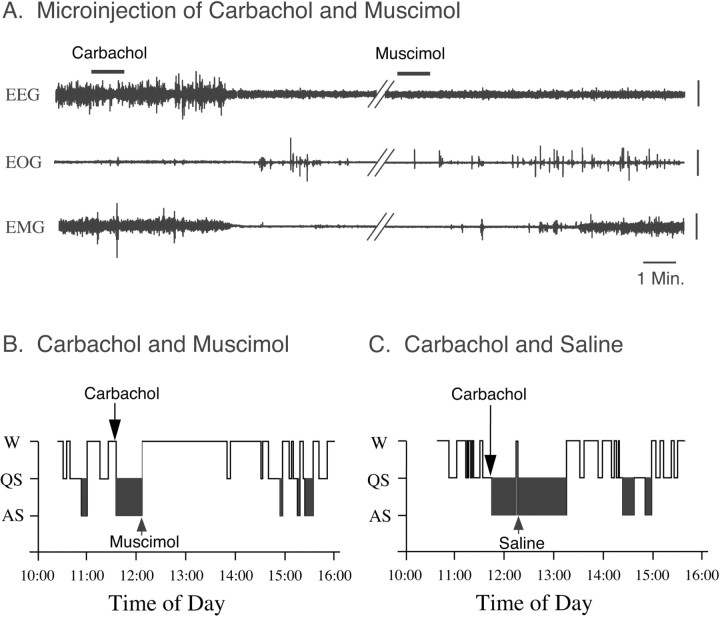
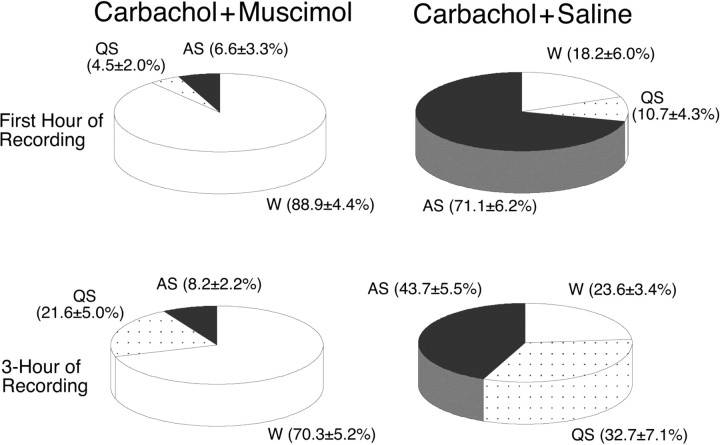
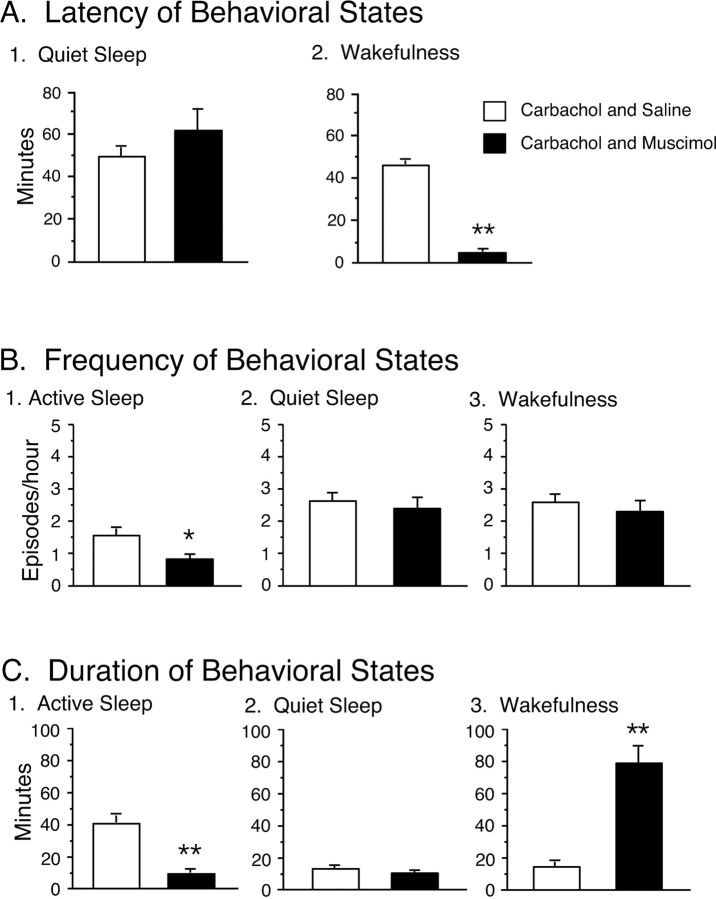
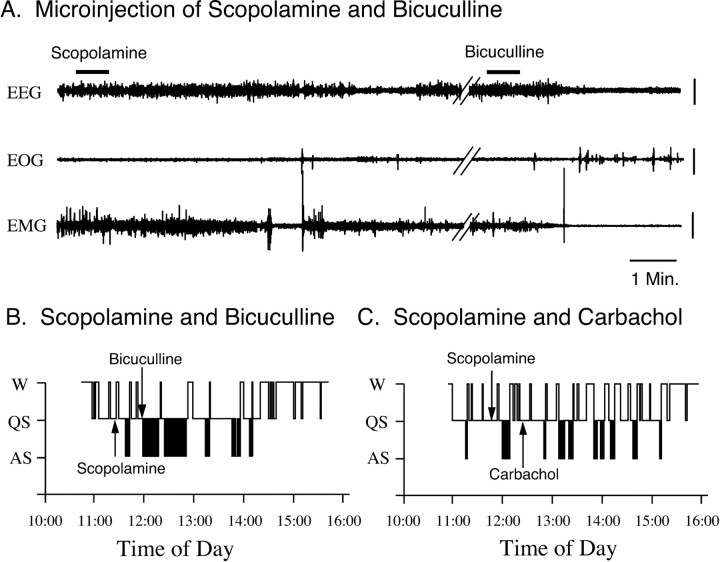
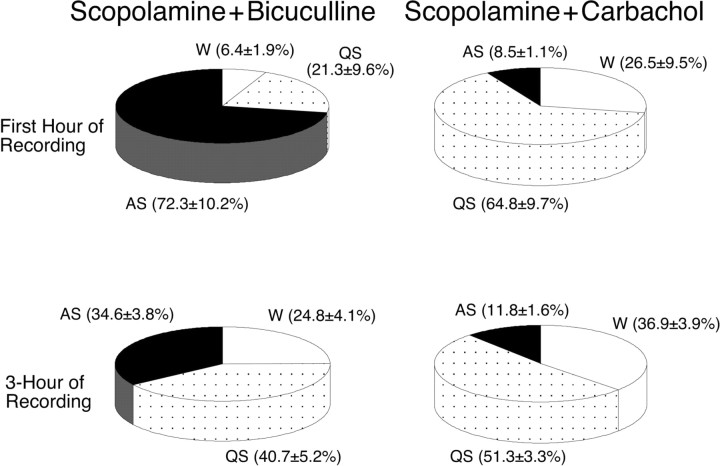
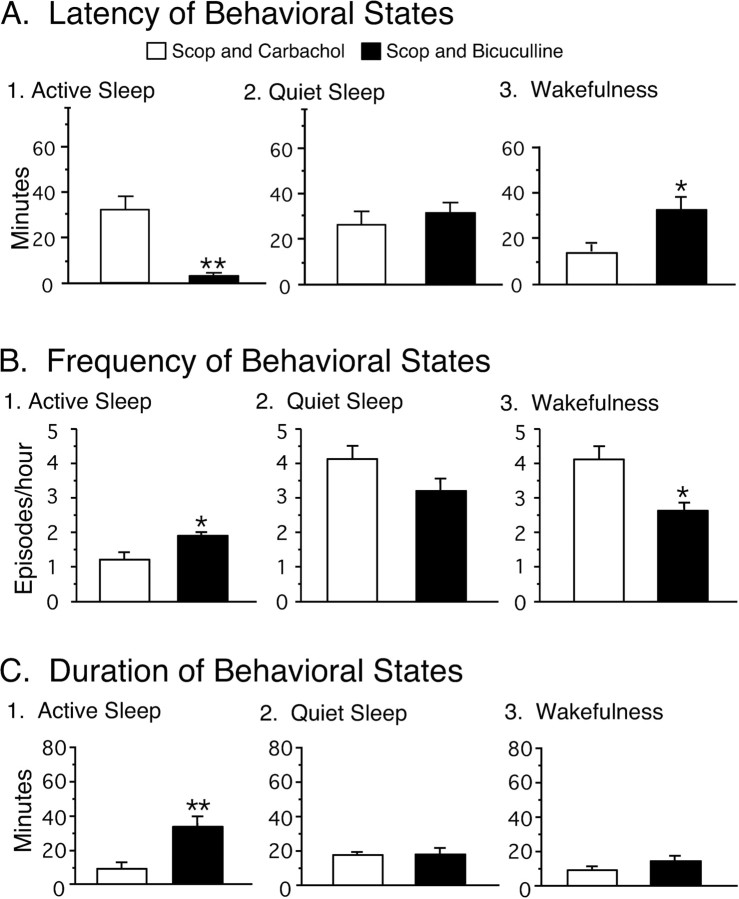
The cholinergic system within the nucleus pontis oralis (NPO) of the pontine tegmentum is critically involved in the generation of active (rapid eye movement) sleep. Previously, we demonstrated that a GABAergic system in the NPO also plays an important role in the control of the behavioral states of wakefulness as well as active sleep. The present study examined interactions between these two neuronal systems vis-a-vis the occurrence of these behavioral states. Accordingly, cholinergic and GABAergic agonists and antagonists were injected into the NPO, and their combined effects on sleep and waking states of chronic, unanesthetized cats were examined. Microinjections of carbachol into the NPO elicited active sleep with a short latency. However, a preinjection of muscimol (a GABA(A) agonist) completely blocked the active sleep-inducing effects of carbachol. The induction of active sleep by carbachol was also suppressed by a subsequent injection of muscimol. On the other hand, the microinjection of scopolamine (a muscarinic receptor antagonist) did not block the induction of active sleep by bicuculline (a GABA(A) antagonist). We conclude that the excitatory cholinergic control of NPO neurons that are involved in the generation of active sleep is gated by a pontine GABAergic system that exerts its effects postsynaptically by inhibiting NPO neurons, resulting in the suppression of active sleep and the generation of wakefulness. In the absence of the activation of this GABAergic gating mechanism, active sleep occurs. These results reveal that specific interactions between cholinergic and GABAergic processes in the NPO play a critical role in the generation of active sleep and wakefulness.
Figures
Similar articles
-
Induction of wakefulness and inhibition of active (REM) sleep by GABAergic processes in the nucleus pontis oralis.Arch Ital Biol. 2001 Feb;139(1-2):125-45. Arch Ital Biol. 2001. PMID: 11256181
-
A GABAergic pontine reticular system is involved in the control of wakefulness and sleep.Sleep Res Online. 1999;2(2):43-8. Sleep Res Online. 1999. PMID: 11382881
-
GABAergic mechanisms in the pedunculopontine tegmental nucleus of the cat promote active (REM) sleep.Brain Res. 2002 Jul 19;944(1-2):1-9. doi: 10.1016/s0006-8993(02)02475-7. Brain Res. 2002. PMID: 12106660
-
Pontine cholinergic mechanisms and their impact on respiratory regulation.Respir Physiol Neurobiol. 2004 Nov 15;143(2-3):235-49. doi: 10.1016/j.resp.2004.04.017. Respir Physiol Neurobiol. 2004. PMID: 15519558 Review.
-
Carbachol models of REM sleep: recent developments and new directions.Arch Ital Biol. 2001 Feb;139(1-2):147-68. Arch Ital Biol. 2001. PMID: 11256182 Review.
Cited by
-
Blockade of GABA, type A, receptors in the rat pontine reticular formation induces rapid eye movement sleep that is dependent upon the cholinergic system.Neuroscience. 2008 Sep 22;156(1):1-10. doi: 10.1016/j.neuroscience.2008.06.067. Epub 2008 Jul 23. Neuroscience. 2008. PMID: 18706488 Free PMC article.
-
Control of sleep and wakefulness.Physiol Rev. 2012 Jul;92(3):1087-187. doi: 10.1152/physrev.00032.2011. Physiol Rev. 2012. PMID: 22811426 Free PMC article. Review.
-
Activity of pontine A7 noradrenergic neurons is suppressed during REM sleep.J Appl Physiol (1985). 2022 Jul 1;133(1):130-143. doi: 10.1152/japplphysiol.00771.2021. Epub 2022 May 26. J Appl Physiol (1985). 2022. PMID: 35616303 Free PMC article.
-
Microinjection of 70-kDal heat shock protein into the oral reticular nucleus of the pons suppresses rapid eye movement sleep in pigeons.Neurosci Behav Physiol. 2009 Mar;39(3):289-96. doi: 10.1007/s11055-009-9132-8. Epub 2009 Feb 21. Neurosci Behav Physiol. 2009. PMID: 19234793
-
Differential localization of carbachol- and bicuculline-sensitive pontine sites for eliciting REM sleep-like effects in anesthetized rats.J Sleep Res. 2009 Mar;18(1):99-112. doi: 10.1111/j.1365-2869.2008.00687.x. Epub 2008 Oct 21. J Sleep Res. 2009. PMID: 19021854 Free PMC article.
References
-
- Amatruda III TT, Black DA, McKenna TM, McCarley RW, Hobson JA (1975) Sleep cycle control and cholinergic mechanisms: differential effects of carbachol injections at pontine brain stem sites. Brain Res 98: 501-515. - PubMed
-
- Baghdoyan HA (1997) Cholinergic mechanisms regulating REM sleep. In: Sleep sciences: integrating basic research and clinical practice. Monographs in clinical neuroscience (Schwartz WJ, ed), pp 88-116. Basel: Karger.
-
- Baghdoyan HA, Rodrigo-Angulo ML, McCarley RW, Hobson JA (1984) Site-specific enhancement and suppression of desynchronized sleep signs following cholinergic stimulation of three brain-stem region. Brain Res 306: 39-52. - PubMed
-
- Baghdoyan HA, Lydic R, Callaway CW, Hobson JA (1989) The carbachol-induced enhancement of desynchronized sleep signs is dose dependent and antagonized by centrally administered atropone. Neuropsychopharmacology 2: 67-69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous