

Prospective evaluation of an internet-linked handheld computer critical care knowledge access system
- PMID: 15566586
- PMCID: PMC1065064
- DOI: 10.1186/cc2967
Prospective evaluation of an internet-linked handheld computer critical care knowledge access system
Abstract
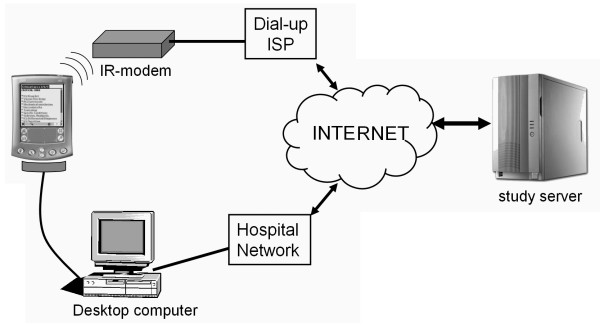
Introduction: Critical care physicians may benefit from immediate access to medical reference material. We evaluated the feasibility and potential benefits of a handheld computer based knowledge access system linking a central academic intensive care unit (ICU) to multiple community-based ICUs.
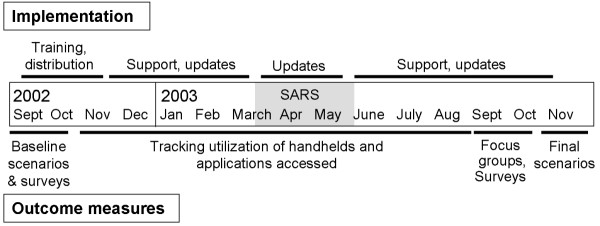
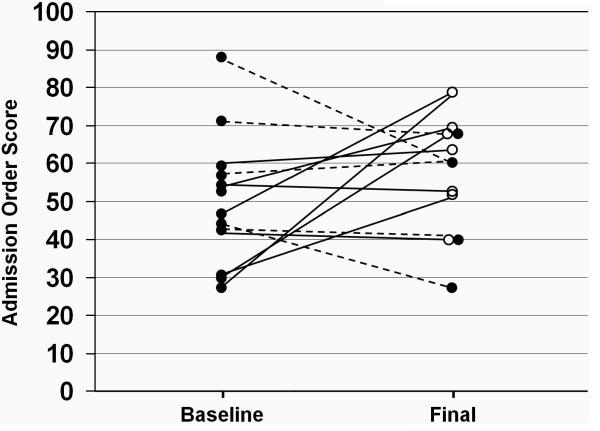
Methods: Four community hospital ICUs with 17 physicians participated in this prospective interventional study. Following training in the use of an internet-linked, updateable handheld computer knowledge access system, the physicians used the handheld devices in their clinical environment for a 12-month intervention period. Feasibility of the system was evaluated by tracking use of the handheld computer and by conducting surveys and focus group discussions. Before and after the intervention period, participants underwent simulated patient care scenarios designed to evaluate the information sources they accessed, as well as the speed and quality of their decision making. Participants generated admission orders during each scenario, which were scored by blinded evaluators.
Results: Ten physicians (59%) used the system regularly, predominantly for nonmedical applications (median 32.8/month, interquartile range [IQR] 28.3-126.8), with medical software accessed less often (median 9/month, IQR 3.7-13.7). Eight out of 13 physicians (62%) who completed the final scenarios chose to use the handheld computer for information access. The median time to access information on the handheld handheld computer was 19 s (IQR 15-40 s). This group exhibited a significant improvement in admission order score as compared with those who used other resources (P = 0.018). Benefits and barriers to use of this technology were identified.
Conclusion: An updateable handheld computer system is feasible as a means of point-of-care access to medical reference material and may improve clinical decision making. However, during the study, acceptance of the system was variable. Improved training and new technology may overcome some of the barriers we identified.
Figures
Similar articles
-
Assessing medical residents' usage and perceived needs for personal digital assistants.Int J Med Inform. 2004 Feb;73(1):25-34. doi: 10.1016/j.ijmedinf.2003.12.005. Int J Med Inform. 2004. PMID: 15036076
-
Pilot study of a web-based antibiotic decision management guide.J Am Coll Surg. 2006 Mar;202(3):459-67. doi: 10.1016/j.jamcollsurg.2005.11.010. Epub 2006 Jan 19. J Am Coll Surg. 2006. PMID: 16500251 Clinical Trial.
-
Use of personal digital assistants (PDAs) in reflection on learning and practice.J Contin Educ Health Prof. 2007 Fall;27(4):227-33. doi: 10.1002/chp.142. J Contin Educ Health Prof. 2007. PMID: 18085601
-
A review and a framework of handheld computer adoption in healthcare.Int J Med Inform. 2005 Jun;74(5):409-22. doi: 10.1016/j.ijmedinf.2005.03.001. Epub 2005 Apr 12. Int J Med Inform. 2005. PMID: 15893264 Review.
-
Use of handheld devices in critical care.Crit Care Nurs Clin North Am. 2005 Mar;17(1):45-50, x. doi: 10.1016/j.ccell.2004.09.006. Crit Care Nurs Clin North Am. 2005. PMID: 15749401 Review.
Cited by
-
Barriers and facilitators to clinical information seeking: a systematic review.J Am Med Inform Assoc. 2019 Oct 1;26(10):1129-1140. doi: 10.1093/jamia/ocz065. J Am Med Inform Assoc. 2019. PMID: 31127830 Free PMC article.
-
Systematic review of factors influencing the adoption of information and communication technologies by healthcare professionals.J Med Syst. 2012 Feb;36(1):241-77. doi: 10.1007/s10916-010-9473-4. Epub 2010 Mar 30. J Med Syst. 2012. PMID: 20703721 Free PMC article.
References
-
- Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troche G, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862–871. doi: 10.1001/jama.288.7.862. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
