

Clinical review: how to optimize management of high-risk surgical patients
- PMID: 15566623
- PMCID: PMC1065048
- DOI: 10.1186/cc2922
Clinical review: how to optimize management of high-risk surgical patients
Abstract
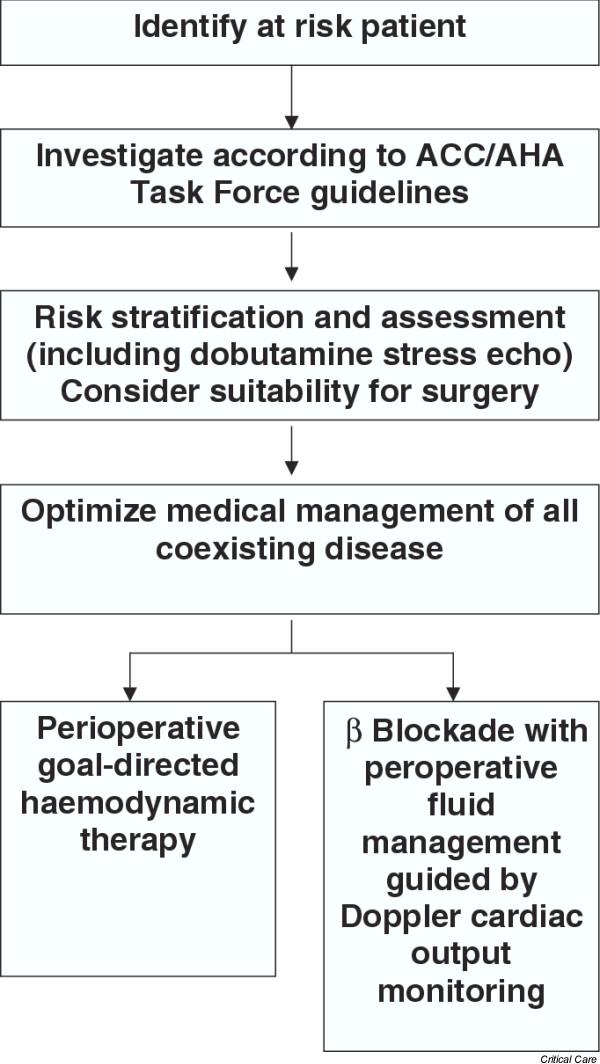
For many patients optimal perioperative care may require little or no additional medical management beyond that given by the anaesthetist and surgeon. However, the continued existence of a group of surgical patients at high risk for morbidity and mortality indicates an ongoing need to identify such patients and deliver optimal care throughout the perioperative period. A group of patients exists in whom the risk for death and serious complications after major surgery is in excess of 20%. The risk is related mainly to the patient's preoperative physiological condition and, in particular, the cardiovascular and respiratory reserves. Cardiovascular management of the high-risk surgical patient is of particular importance. Once the medical management of underlying disease has been optimized, two principal areas remain: the use of haemodynamic goals to guide fluid and inotropic therapy, and perioperative beta blockade. A number of studies have shown that the use of goal-directed haemodynamic therapy during the perioperative period can result in large reductions in morbidity and mortality. Some patients may also benefit from perioperative beta blockade, which in selected patients has also been shown to result in significant mortality reductions. In this review a pragmatic approach to perioperative management is described, giving guidance on the identification of the high-risk patient and on the use of goal-directed haemodynamic therapy and beta blockade.
Figures
References
-
- Shoemaker WC. Cardiorespiratory patterns of surviving and nonsurviving postoperative patients. Surg Gynecol Obstet. 1972;134:810–814. - PubMed
-
- Clowes GH, Del Guercio LR. Circulatory response to trauma of surgical operations. Metabolism. 1960;9:67–81. - PubMed
-
- Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–1186. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
