

CNS MR and CT findings associated with a clinical presentation of herpetic acute retinal necrosis and herpetic retrobulbar optic neuritis: five HIV-infected and one non-infected patients
- PMID: 15569737
- PMCID: PMC8148741
CNS MR and CT findings associated with a clinical presentation of herpetic acute retinal necrosis and herpetic retrobulbar optic neuritis: five HIV-infected and one non-infected patients
Abstract
Introduction: This report demonstrates the spectrum of central nervous system (CNS) abnormalities observed on MR imaging and CT studies in 6 patients with clinical or pathologic diagnoses of acute retinal necrosis (ARN) and retrobulbar optic neuritis (RBON-H) resulting from Herpes Zoster Virus and Cytomegalovirus. We discuss the etiologic and pathophysiologic implications regarding these findings.
Methods: Standard MR imaging sequences of the whole brain and selected high-resolution images of the orbits and globes, from 6 patients, were reviewed by three neuroradiologists for consensus interpretation of the findings. Special sequences augmenting disease were obtained in individual cases. Axial CT images were obtained from two patients using 5mm sequential slices.
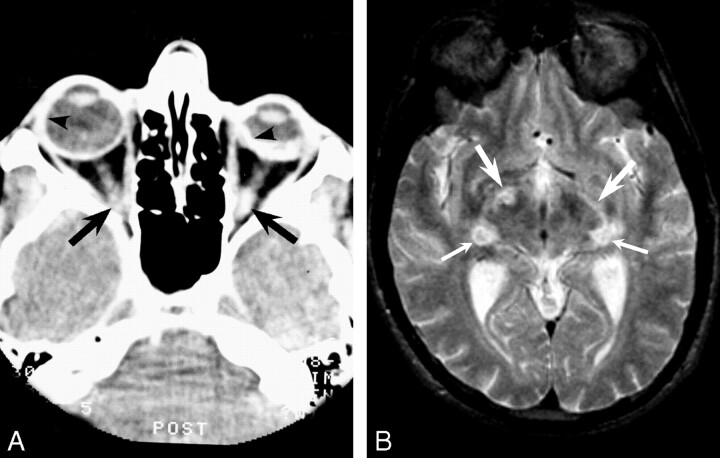
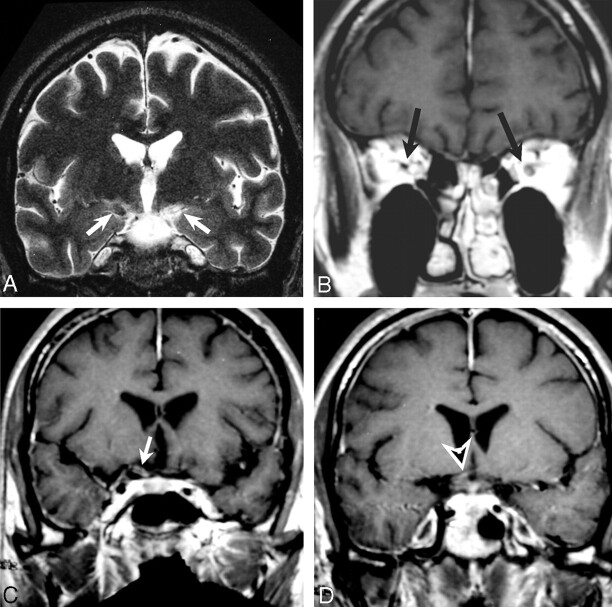
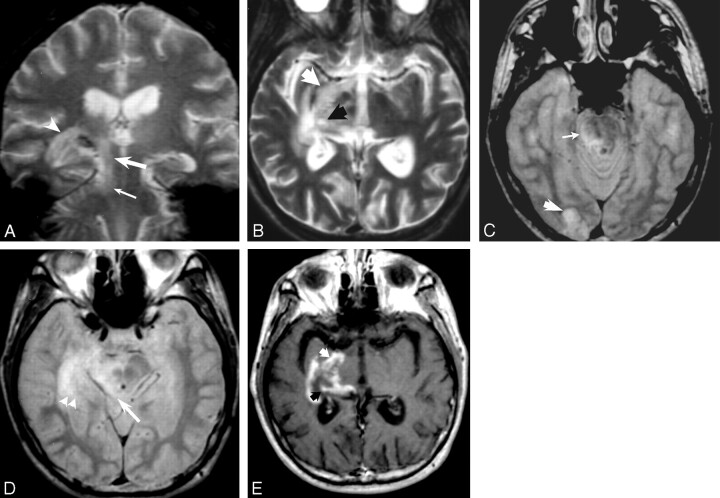
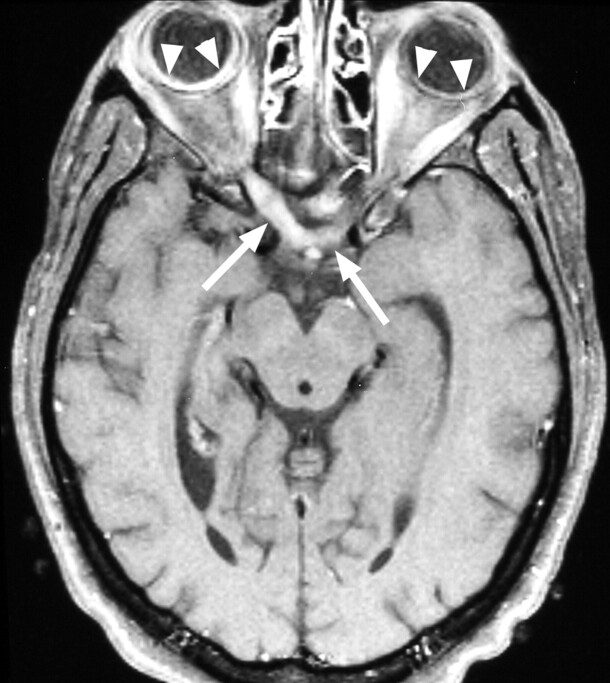
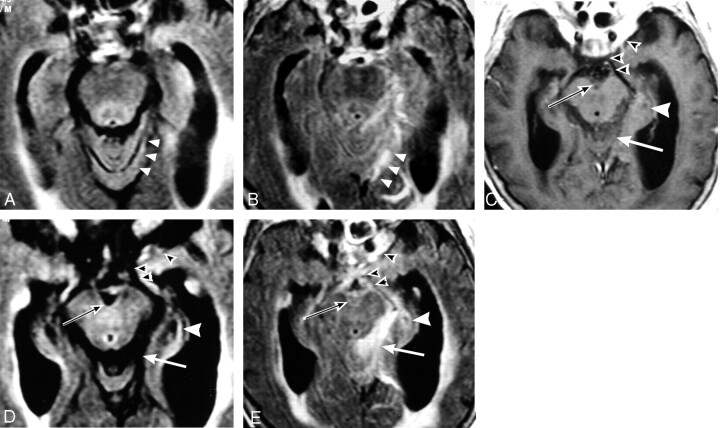
Results: MR imaging findings showed both T2 signal brightening and contrast enhancement in one or both optic nerves, optic tracts and lateral geniculate bodies, as well as the postsynaptic optic radiations and optic cortex. Similar findings were observed in the superior colliculus, lateral midbrain and cerebellum, with multiple potential etiologic possibilities regarding pathways of dissemination. Low T2* signal (indicating magnetic field susceptibility effects) and CT hyperdensity, consistent with prior hemorrhage, were also observed in the optic tracts, optic radiations and lateral geniculate bodies. Post-contrast enhancement was observed in the meninges and Meckle's cave in one HIV negative patient.
Conclusion: These cases demonstrate CNS imaging findings associated with RBON that are temporally-related to ARN. They support the hypothesis that RBON can either precede or follow ARN and implicate transneuronal, transsynaptic and/or transcerebrospinal fluid viral spread by the herpetic family.
Figures
References
-
- Litoff D, Catalano RA. Herpes zoster optic neuritis in human immunodeficiency virus infection. Arch Ophthalmol 1990;108:782–783 - PubMed
-
- Selbst RG, Selhorst JB., Harbison JW, Myer EC. Parainfectious optic neuritis: report and review following varicella. Arch Neurol 1983;40:347–350 - PubMed
-
- Kuppermann BD, Quiceno JI, Wiley C, et al. Clinical and histopathologic study of varicella zoster virus retinitis in patients with the acquired immunodeficiency syndrome. Am J Ophthalmol 1994;188:589–600 - PubMed
-
- Mansour AM. Neuro-ophthalmic findings in acquired immunodeficiency syndrome. J Clin Neuro-Ophthalmol 1990;10:167–174 - PubMed
-
- Garweg J, Bohnke M. Varicella-zoster virus is strongly associated with atypical necrotizing herpetic retinopathies. Clin Infect Dis 1997;24:603–608 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical