

Treatment of internal carotid artery aneurysms with a covered stent: experience in 24 patients with mid-term follow-up results
- PMID: 15569740
- PMCID: PMC8148739
Treatment of internal carotid artery aneurysms with a covered stent: experience in 24 patients with mid-term follow-up results
Abstract
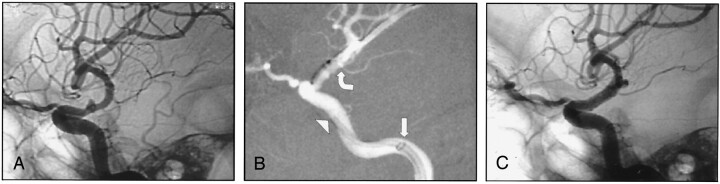
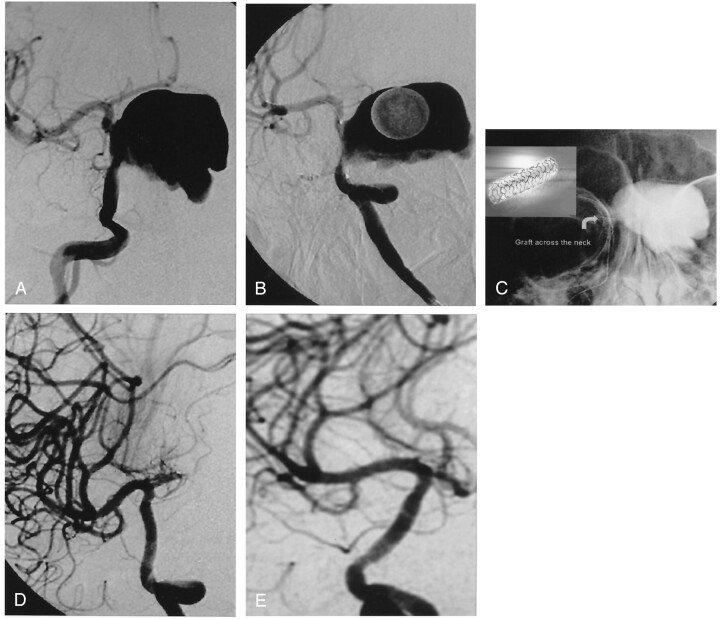
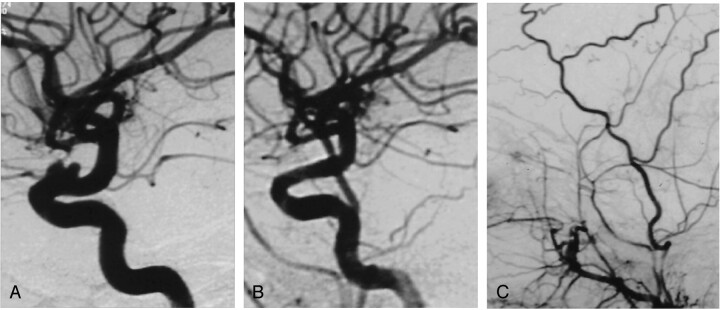
Background and purpose: We present our preliminary experience, including mid-term angiographic and clinical follow-up results, with an alternative technique for the endovascular treatment of intracranial aneurysms in a series of patients. This new method, previously described in anecdotal case reports, consists of endovascular deployment of an artificial vessel graft (stent graft or covered stent) in the parent vessel to exclude the intracranial aneurysm sac from circulation.
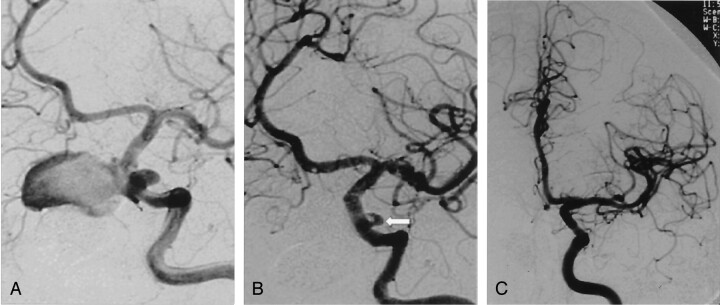
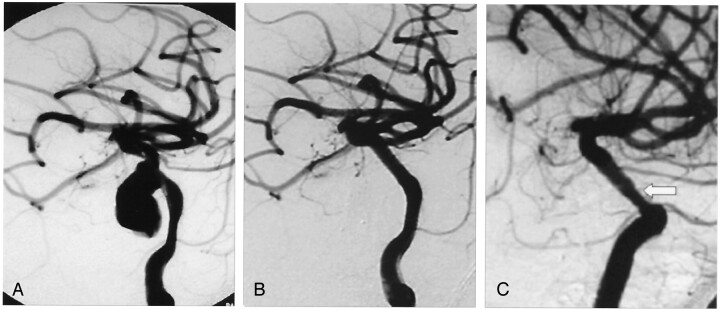
Methods: Twenty-five internal carotid artery (ICA) aneurysms in 24 patients were successfully treated by using a Jostent coronary stent graft deployed in the parent artery across the aneurysm neck. All except four aneurysms were extradural, located in the petrous or cavernous portion of the ICA. The four intradural aneurysms were located in the carotico-ophthalmic region. Seventeen aneurysms in 16 patients occurred posttraumatically, secondary to motor vehicle accidents or surgical injury.
Results: Twenty-three aneurysms were immediately excluded from circulation after stent graft placement. In two aneurysms, a slow contrast material filling (endoleak) into the aneurysm cavity was observed immediately after treatment. One was thrombosed, as shown by late control angiography; in the other one, a second larger bare stent was used to appose the stent graft's distal end to the ICA wall, thus sealing the endoleak into the distal graft. No technical adverse event, including vessel dissection, vessel perforation, or thromboembolism, occurred with or without clinical consequence. No mortality or morbidity developed during or after the procedure, including the follow-up period. Two-year control angiography in one patient, 1.5-year control angiography in two patients, 1-year control angiography in six patients, and 6-month control angiography in 12 patients were performed, revealing reconstruction of the ICA with no aneurysm recanalization. All symptoms resolved after treatment in the patients who had initially presented with mass effect.
Conclusion: Initial anatomic, clinical and mid-term follow-up results in this small series of patients are encouraging. This technique has been proved to have potential in the reconstructive treatment of intracranial aneurysms. Further research and development are needed to optimize the stent graft technology for the cerebrovascular system.
Figures
Similar articles
-
Application of the Willis covered stent in the treatment of aneurysm in the cisternal segment of the internal carotid artery: a pilot comparative study with midterm follow-up.J Endovasc Ther. 2010 Feb;17(1):55-65. doi: 10.1583/09-2688.1. J Endovasc Ther. 2010. PMID: 20199268
-
A single-center experience in the endovascular treatment of carotid siphon aneurysms using the Willis covered stent: a retrospective analysis.J Neurointerv Surg. 2018 Dec;10(12):1197-1202. doi: 10.1136/neurintsurg-2017-013695. Epub 2018 Apr 21. J Neurointerv Surg. 2018. PMID: 29680819
-
Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms.J Neurosurg. 1999 Oct;91(4):538-46. doi: 10.3171/jns.1999.91.4.0538. J Neurosurg. 1999. PMID: 10507372
-
Multiple overlapping stents as monotherapy in the treatment of 'blister' pseudoaneurysms arising from the supraclinoid internal carotid artery: a single institution series and review of the literature.J Neurointerv Surg. 2014 Apr 1;6(3):184-94. doi: 10.1136/neurintsurg-2013-010648. Epub 2013 Mar 30. J Neurointerv Surg. 2014. PMID: 23543733 Review.
-
Transradial Stent-Assisted Coiling Using "Dual-Jailing" Technique for Kissing Aneurysms of the Internal Carotid Artery: Technical Note and Literature Review.World Neurosurg. 2023 Feb;170:175-181. doi: 10.1016/j.wneu.2022.11.018. Epub 2022 Nov 8. World Neurosurg. 2023. PMID: 36368455 Review.
Cited by
-
Pseudoaneurysm of the Petrosal Internal Carotid Artery in the Middle Ear as a Complication of Middle Ear Cholesteatoma.J Audiol Otol. 2015 Apr;19(1):58-61. doi: 10.7874/jao.2015.19.1.58. Epub 2015 Apr 17. J Audiol Otol. 2015. PMID: 26185794 Free PMC article.
-
Internal carotid artery false aneurysm as a fatal complication of transsphenoidal surgery.J Surg Case Rep. 2021 Apr 22;2021(4):rjab146. doi: 10.1093/jscr/rjab146. eCollection 2021 Apr. J Surg Case Rep. 2021. PMID: 33927876 Free PMC article.
-
Intracranial pseudoaneurysms, fusiform aneurysms and carotid-cavernous fistulas. Repair with percutaneous implantation of endovascular covered stents.Interv Neuroradiol. 2008 Dec 29;14(4):435-40. doi: 10.1177/159101990801400409. Epub 2009 Jan 5. Interv Neuroradiol. 2008. PMID: 20557743 Free PMC article.
-
Endovascular graft-stent placement for treatment of traumatic carotid cavernous fistulas.J Korean Neurosurg Soc. 2009 Dec;46(6):572-6. doi: 10.3340/jkns.2009.46.6.572. Epub 2009 Dec 31. J Korean Neurosurg Soc. 2009. PMID: 20062575 Free PMC article.
-
Treatment of carotid siphon aneurysms by use of the Willis stent graft: an angiographic and histopathological study.Eur Radiol. 2010 Aug;20(8):1974-84. doi: 10.1007/s00330-010-1738-2. Epub 2010 Mar 20. Eur Radiol. 2010. PMID: 20306085
References
-
- International Subarachnoid Aneurysm Trial (ISAT) Colloborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomized trial. Lancet 2002;360:1267–1274 - PubMed
-
- Gruber A, Killer M, Bavinzski G, Richling B. Clinical and angiographic results of endovascular coiling treatment of giant and very large intracranial aneurysms: a 7-year, single-center experience. Neurosurgery 1999;45:793–804 - PubMed
-
- Kattner KA, Bailes J, Fukushima T. Direct surgical management of large bulbous and giant aneurysms involving the paraclinoid segment of the internal carotid artery: report of 29 cases. Surg Neurol 1998;49:471–480 - PubMed
-
- Moret J, Cognard C, Weill A, Castaings L, Rey A. Reconstruction technique in the treatment of wide-neck intracranial aneurysms: long-term angiographic and clinical results: apropos of 56 cases [in French]. J Neuroradiol 1997;24:30–44 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous