

Thromboembolic events associated with balloon-assisted coil embolization: evaluation with diffusion-weighted MR imaging
- PMID: 15569744
- PMCID: PMC8148712
Thromboembolic events associated with balloon-assisted coil embolization: evaluation with diffusion-weighted MR imaging
Abstract
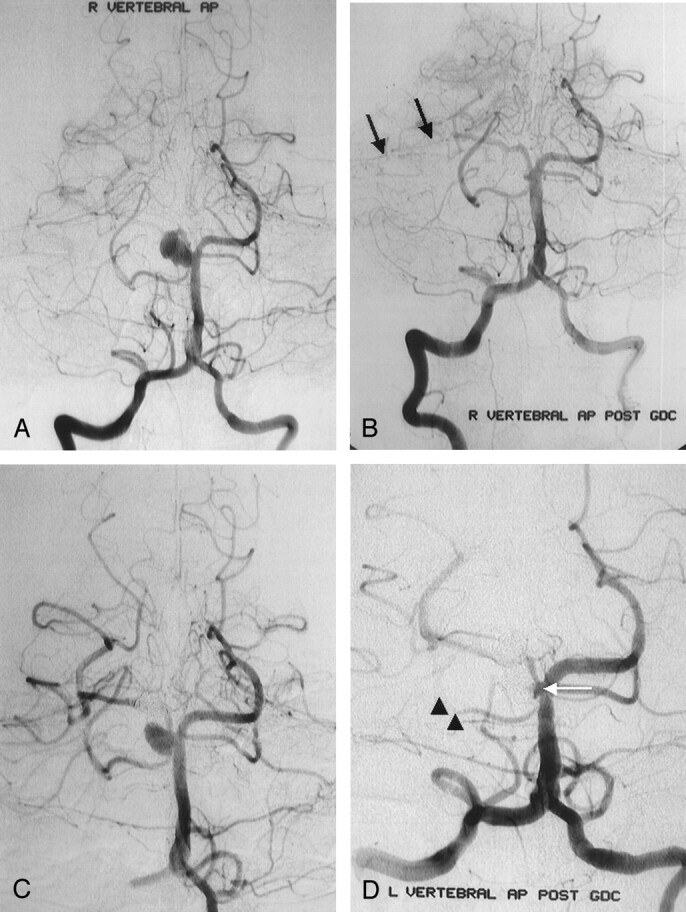
Background and purpose: Thromboembolic events may occur during or after the treatment of intracranial aneurysms with Guglielmi detachable coils (GDCs). The purpose of this study was to determine the frequency of thromboembolic events associated with balloon-assisted coil placement and to investigate possible risk factors for these events during balloon-assisted coil placement and embolization.
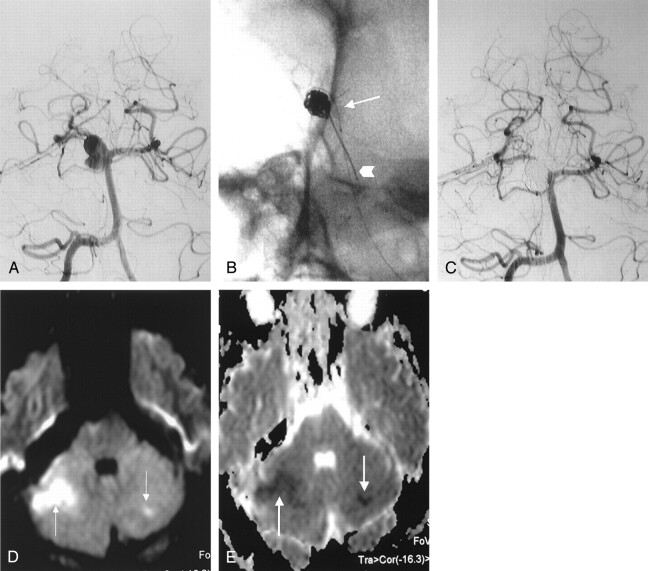
Methods: Twenty patients with cerebral aneurysms treated with balloon-assisted coil placement and embolization at our institution were included. All patients underwent diffusion-weighted (DW) imaging within 6 hours after the procedure. Two neuroradiologists reviewed all DW images to detect ischemic lesions.
Results: Hyperintense lesions compatible with thromboembolic events were detected on DW images of four (20%) patients. Three lesions were in the territory of posterior circulation, and one was in the territory of anterior circulation. The occurrence of new lesions was strongly associated with the number of times the microcatheter or coil was repositioned and removed and with the size of the aneurysmal neck (P < .01). DW imaging findings did not suggest a strong correlation between the occurrence of new ischemic lesions and potential risk factors (maximum balloon inflation time, number of times the balloon was inflated, etc.) associated with balloon-assisted coil placement and embolization (P > .05).
Conclusion: The risk of thromboembolic events during the treatment of intracranial aneurysms with balloon-assisted techniques is not more significant than when conventional GDC techniques are used. The only variables found to influence this risk during or after balloon-assisted coil placement were microcatheter repositioning, coil removal and repositioning, and size of the aneurysmal neck.
Figures
References
-
- Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, I: electrochemical basis, technique and experimental results. J Neurosurg 1991;75:1–7 - PubMed
-
- Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, 2: preliminary clinical experience. J Neurosurg 1991;75:8–14 - PubMed
-
- Nichols DA, Meyer FB, Piepgras DG, Smith PL. Endovascular treatment of intracranial aneurysms: subject review. Mayo Clin Proc 1994;69:272–285 - PubMed
-
- Moret J, Cognard C, Weill A, Castaings L, Rey A. The “remodeling technique” in the treatment of wide neck intracranial aneurysms: Angiographic results and clinical follow-up in 56 cases. Intervent Neuroradiol 1997;3:21–35 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical