

Evolution of donor morbidity in living related liver transplantation: a single-center analysis of 165 cases
- PMID: 15570207
- PMCID: PMC1356517
- DOI: 10.1097/01.sla.0000146146.97485.6c
Evolution of donor morbidity in living related liver transplantation: a single-center analysis of 165 cases
Abstract
Objective: During the last 14 years, living donor liver transplantation (LDLT) has evolved to an indispensable surgical strategy to minimize mortality of adult and pediatric patients awaiting transplantation. The crucial prerequisite to performing this procedure is a minimal morbidity and mortality risk to the healthy living donor. Little is known about the learning curve involved with this type of surgery.
Patients and methods: From January 1991 to August 2003, a total of 165 LDLTs were performed in our center. Of these, 135 were donations of the left-lateral lobe (LL, segments II and III), 3 were of the left lobe (L, segments II-IV), 3 were full-left lobes (FL, segments I-IV), and 24 were of the full-right lobe (FR, segments V-VIII). We divided the procedures into 3 periods: period 1 included the years 1991 to 1995 (LL, n = 49; L, n = 2; FR, n = 1), period 2 covered 1996 to 2000 (LL, n = 47), and period 3 covered 2001 to August 2003 (LL, n = 39; FR, n = 23; FL, n = 3; L, n = 1). Perioperative mortality and morbidity were assessed using a standardized classification. Length of stay in intensive care unit, postoperative hospital stay, laboratory results (bilirubin, INR, and LFTs), morbidity, and the different types of grafts in the 3 different periods were compared.
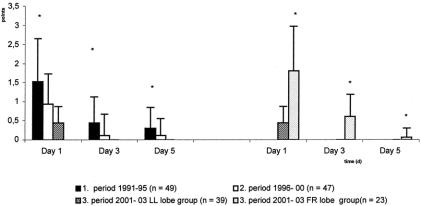
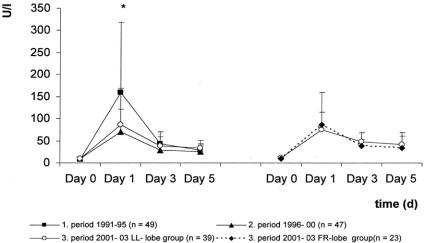
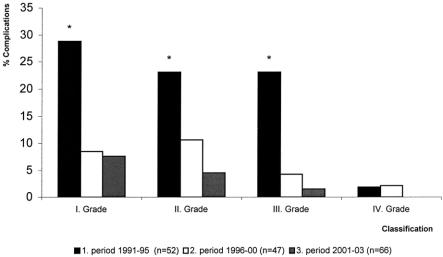
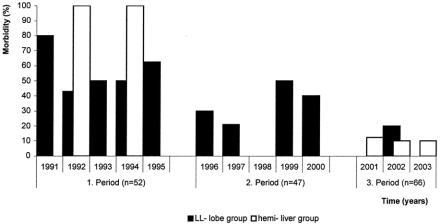
Results: One early donor death was observed in period 1 (03/07/93, case 30; total mortality, 0.61.%). Since 1991, the perioperative morbidity has continually declined (53.8% vs. 23.4% vs. 9.2%). In period 1, 28 patients had 40 complications. In period 2, 11 patients had 12 complications, and in period 3, 6 patients had 9 complications. Within the first period, 1 donor underwent relaparotomy because of bile leakage. Postoperative hospital stay was 10 days, 7 days, and 6 days, respectively. Donation of the full right lobe, in comparison with that of the left lateral lobe, resulted in a significantly diminished liver function (bilirubin and INR) during the first 5 days after donation but did not increase morbidity. One donor from period 1 experienced late death caused by amyotrophic lateral sclerosis.
Conclusions: In a single center, morbidity after living liver donation strongly correlates to center experience. Despite the additional risks associated with temporary reduction of liver function, this experience enabled the team to bypass part of the learning curve when starting right lobe donation. Specific training of the surgical team and coaching by an experienced center should be implemented for centers offering this procedure to avoid the learning curve.
Figures
References
-
- Raia S, Nery JR, Mies S. Liver transplantation from live donors. Lancet. 1989;2:497. - PubMed
-
- Strong RW, Lynch SV, Ong TH, et al. Successful liver transplantation from a living donor to her son. N Engl J Med. 1990;322:1505–1507. - PubMed
-
- Emond JC, Whitington PF, Thistlethwaite JR, et al. Reduced-size orthotopic liver transplantation: use in the management of children with chronic liver disease. Hepatology. 1989;10:867–872. - PubMed
-
- Malago M, Rogiers X, Broelsch CE. Reduced-size hepatic allografts. Annu Rev Med. 1995;46:507–512. - PubMed
-
- Daar AS. Organ donation—world experience; the Middle East. Transplant Proc. 1991;23:2505–2507. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
