

A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases
- PMID: 15570209
- PMCID: PMC1356519
- DOI: 10.1097/01.sla.0000145965.86383.89
A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases
Abstract
Objective: To assess outcome after a 2-stage hepatectomy procedure (TSHP) combined with portal vein embolization (PVE) in the treatment of patients with unresectable multiple and bilobar colorectal liver metastases (MBCLM).
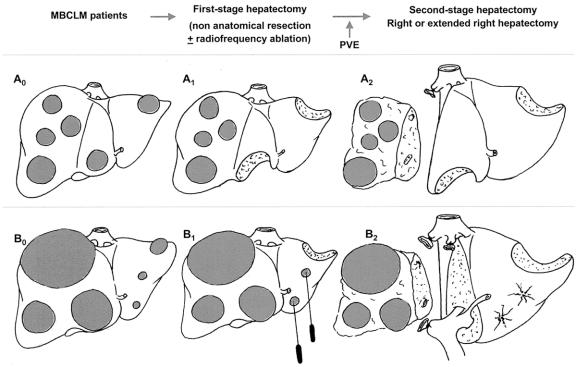
Background: Patients with MBCLM are often considered for palliative chemotherapy only, due to too small future remnant liver (FRL). Recently, right hepatectomy with simultaneous left liver wedge resections after previous right PVE has been reported in a curative intent. However, the growth of metastatic nodules in FRL after PVE can be more rapid than that of the nontumoral remnant hepatic parenchyma. Therefore, metastases located in the FRL should be ideally resected before PVE. Then, a right (or extended right) hepatectomy can be safely performed during a second-stage hepatectomy. Therefore, we analyzed our experience with the use of TSHP combined with PVE in treatment of MBCLM.
Patients and methods: Between December 1996 and April 2003, 33 patients with unresectable MBCLM were selected for a TSHP. A right or an extended right hepatectomy was planned after treatment of left FRL metastases to achieve a curative resection. The first-stage hepatectomy consisted in a clearance of the left hemiliver by resection or radiofrequency destruction of metastases of the left FRL. Subsequently, a right PVE was performed to induce atrophy of the right hemiliver and hypertrophy of the left hemiliver. Finally, a second-stage hepatectomy was planned to resect the right liver metastases.
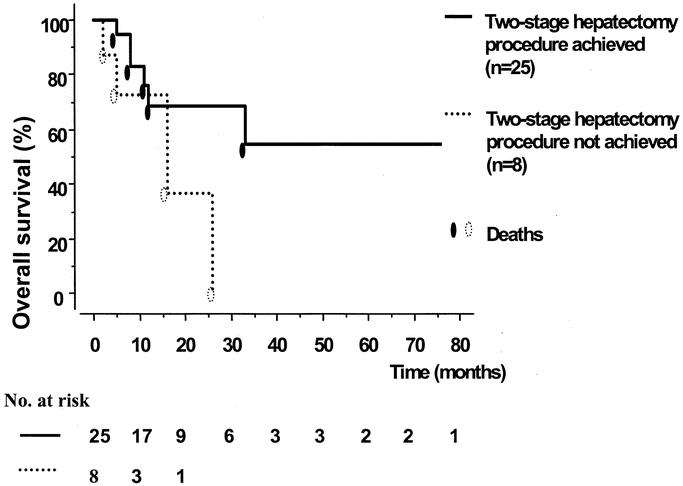
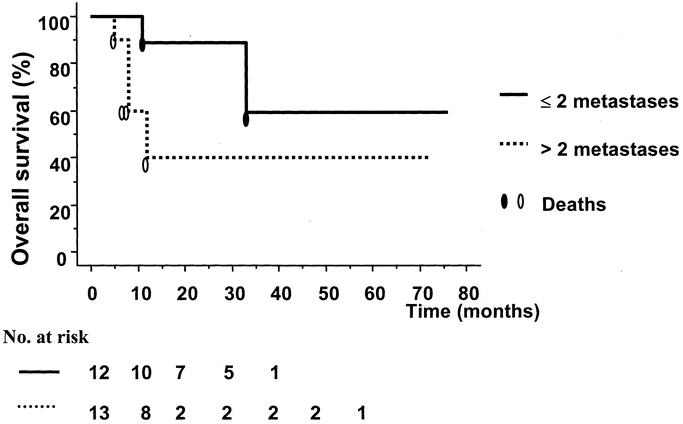
Results: There was no operative mortality. Post-PVE morbidity was 18.1%; postoperative morbidity was 15.1% and 56.0% after first- and second-stage hepatectomy, respectively. TSHP could be achieved in 25 of 33 patients (75.7%). The 1- and 3-year survival rates were 70.0% and 54.4%, respectively, in the 25 patients in whom the TSHP was completed.
Conclusions: In selected patients with initially unresectable MBCLM, a TSHP combined with PVE can be achieved safely with long-term survival similar to that observed in patients with initially resectable liver metastases.
Figures
References
-
- Nordlinger B, Jaeck D, Guiguet M, et al. Surgical resection of hepatic metastases: multicentric retrospective study by the French Association of Surgery. In: Nordlinger B, Jaeck D, eds. Treatment of Hepatic Metastases of Colorectal Cancer. Paris: Springer-Verlag, 1992:129–146.
-
- Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection of colorectal carcinoma metastases to the liver: a prognostic scoring system to improve case selection, based on 1568 patients. Cancer. 1996;77:1254–1262. - PubMed
-
- Jaeck D, Bachellier P, Guiguet M, et al. Long-term survival following resection of colorectal hepatic metastases. Br J Surg. 1997;84:977–980. - PubMed
-
- Scheele J, Stangl R, Altendorf-Hofmann A, et al. Resection of colorectal metastases. World J Surg. 1995;19:59–71. - PubMed
-
- Moertel CG. Chemotherapy for colorectal cancer. N Engl J Med. 1994;330:1136–1139. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
