

Evidence-based value of prophylactic drainage in gastrointestinal surgery: a systematic review and meta-analyses
- PMID: 15570212
- PMCID: PMC1356522
- DOI: 10.1097/01.sla.0000146149.17411.c5
Evidence-based value of prophylactic drainage in gastrointestinal surgery: a systematic review and meta-analyses
Abstract
Objective: To determine the evidence-based value of prophylactic drainage in gastrointestinal (GI) surgery.
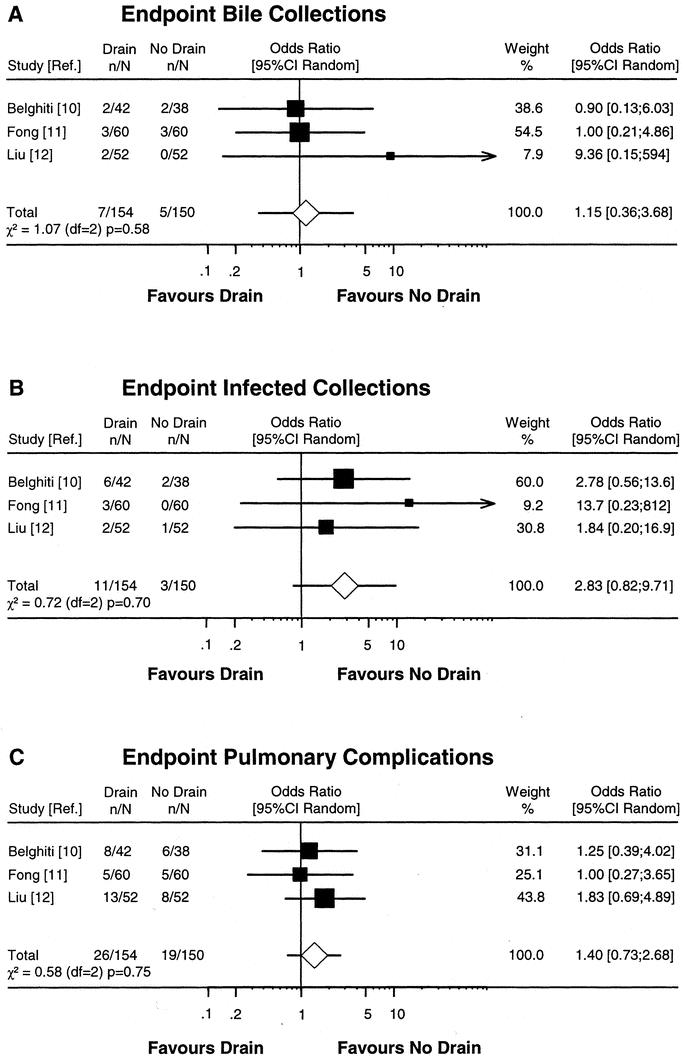
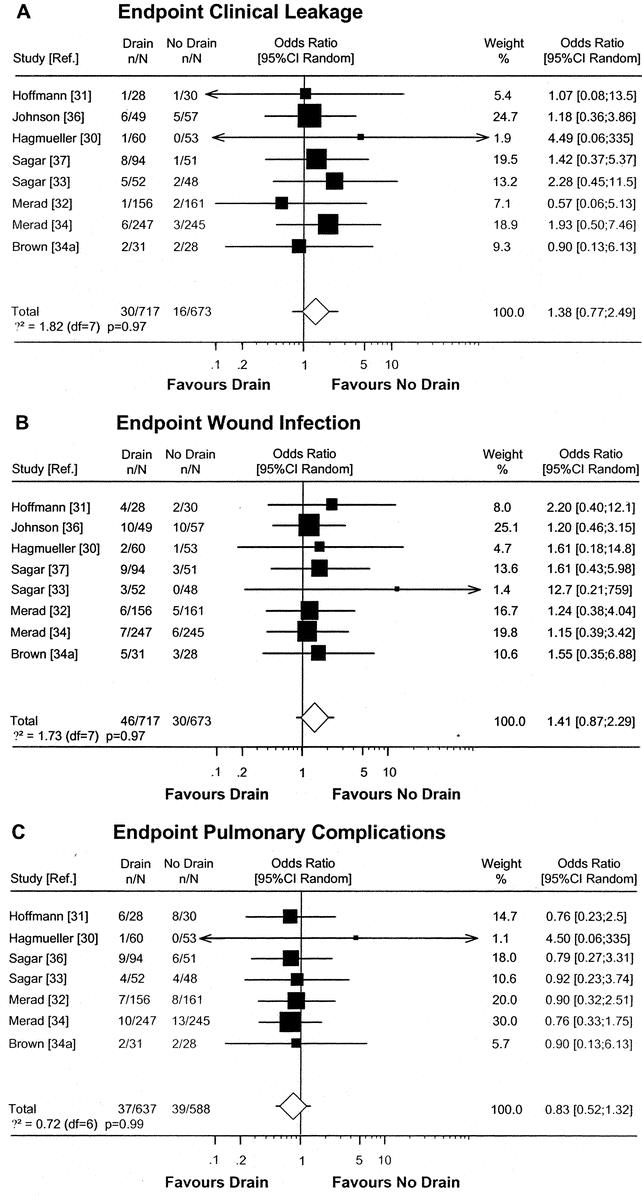
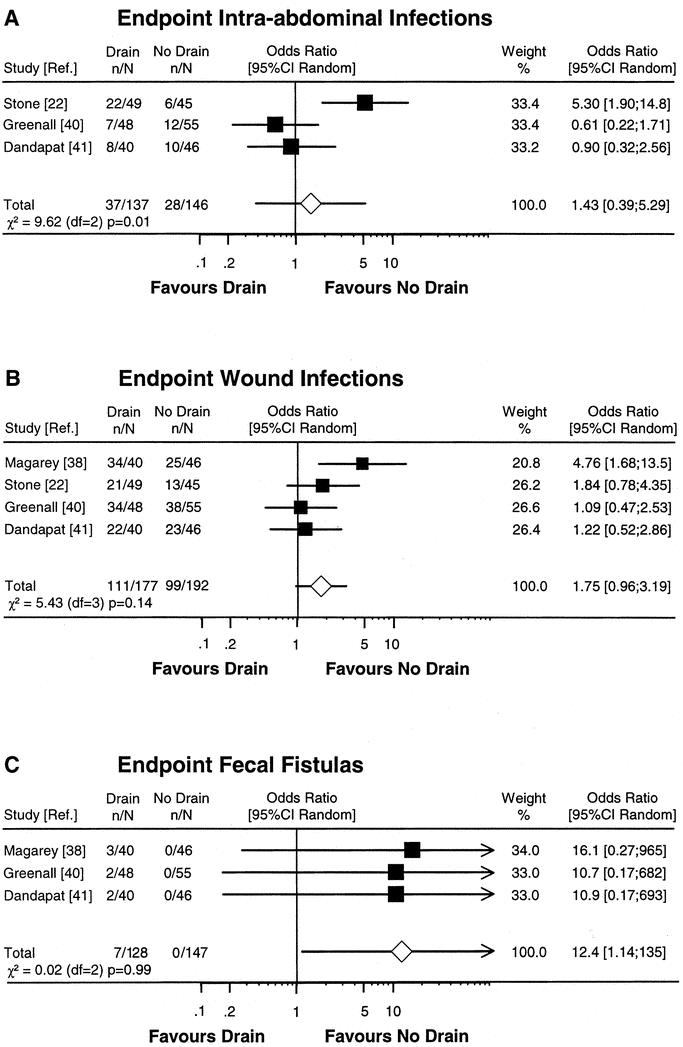
Methods: An electronic search of the Medline database from 1966 to 2004 was performed to identify articles comparing prophylactic drainage with no drainage in GI surgery. The studies were reviewed and classified according to their quality of evidence using the grading system proposed by the Oxford Centre for Evidence-based Medicine. Seventeen randomized controlled trials (RCTs) were found for hepato-pancreatico-biliary surgery, none for upper GI tract, and 13 for lower GI tract surgery. If sufficient RCTs were identified, we performed a meta-analysis to characterize the drain effect using the random-effects model.
Results: There is evidence of level 1a that drains do not reduce complications after hepatic, colonic, or rectal resection with primary anastomosis and appendectomy for any stage of appendicitis. Drains were even harmful after hepatic resection in chronic liver disease and appendectomy. In the absence of RCTs, there is a consensus (evidence level 5) about the necessity of prophylactic drainage after esophageal resection and total gastrectomy due to the potential fatal outcome in case of anastomotic and gastric leakage.
Conclusion: Many GI operations can be performed safely without prophylactic drainage. Drains should be omitted after hepatic, colonic, or rectal resection with primary anastomosis and appendectomy for any stage of appendicitis (recommendation grade A), whereas prophylactic drainage remains indicated after esophageal resection and total gastrectomy (recommendation grade D). For many other GI procedures, especially involving the upper GI tract, there is a further demand for well-designed RCTs to clarify the value of prophylactic drainage.
Figures
References
-
- Robinson JO. Surgical drainage: a historical perspective. Br J Surg. 1986;73:422–426. - PubMed
-
- Dougherty HH, Simmons RL. The biology and practice of surgical drains. Curr Probl Surg. 1992;29:559–730. - PubMed
-
- Billroth T. Clinical Surgery. Translated by Dent CT. London: The New Sydenham Society; 1881.
-
- Delbert P. Recherches experimentelle sur la lavage au peritoneum. Ann Gynekol Obstet. 1889;32:165–197.
-
- Von Ott. Die drainage nach laparotomyie –experimentelle untersuchung. Medicinsky Westnick, No. 1978. Zentralbl Gynaek 1879;3:86–87.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
