

Review
doi: 10.1136/bmj.329.7478.1328.
Tibialis posterior dysfunction: a common and treatable cause of adult acquired flatfoot
Affiliations
- PMID: 15576744
- PMCID: PMC534847
- DOI: 10.1136/bmj.329.7478.1328
Item in Clipboard
Review
Tibialis posterior dysfunction: a common and treatable cause of adult acquired flatfoot
BMJ.
.
No abstract available
Figures
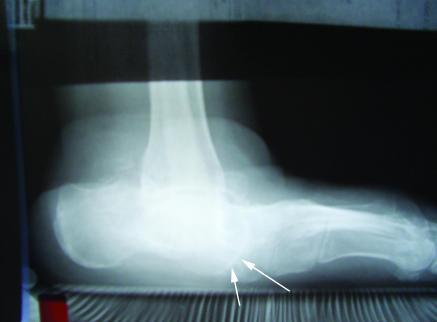
Stage III tibialis posterior dysfunction before and after surgery (a triple arthrodesis). (top) Preoperative film shows a plantar flexed talus (arrows point to head of talus) and loss of arch contour and height. (bottom) Postoperative film shows union and reconstitution of the arch

Stage III tibialis posterior dysfunction before and after surgery (a triple arthrodesis). (top) Preoperative film shows a plantar flexed talus (arrows point to head of talus) and loss of arch contour and height. (bottom) Postoperative film shows union and reconstitution of the arch
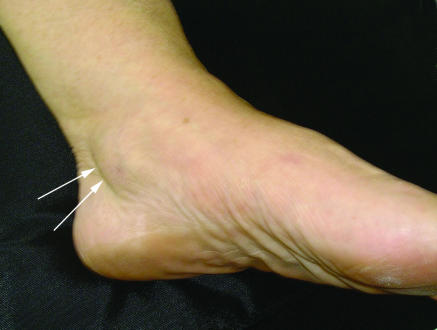
Arrows indicate swelling along the tibialis posterior tendon

Left tibialis posterior dysfunction deformity is easily visible. The medial longitudinal arch is flattened. The left heel is in valgus. Also visible is the “too many toes sign,” which results from abduction of the left forefoot

(top) Unsupported single heel rise on patient's good (right) side. (bottom) Attempt to perform a single heel rise on the affected left side. The patient was unable to do so unsupported but for the purpose of this photo was allowed to lean forward and support herself on the counter in front of her. The heel of the left foot has not inverted into varus

(top) Unsupported single heel rise on patient's good (right) side. (bottom) Attempt to perform a single heel rise on the affected left side. The patient was unable to do so unsupported but for the purpose of this photo was allowed to lean forward and support herself on the counter in front of her. The heel of the left foot has not inverted into varus

Before surgery (top) and five years after surgery (bottom) for a patient with stage II tibialis posterior dysfunction. The surgical reconstruction included a Cobb split tibialis anterior tendon transfer and a Rose varus calcaneal osteotomy

Before surgery (top) and five years after surgery (bottom) for a patient with stage II tibialis posterior dysfunction. The surgical reconstruction included a Cobb split tibialis anterior tendon transfer and a Rose varus calcaneal osteotomy
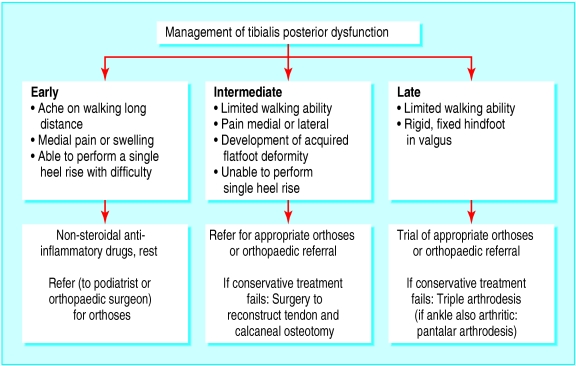
Treating tibialis posterior dysfunction
Similar articles
-
[Tibialis posterior tendon dysfunction. An often neglected cause of painful adult flatfoot].Ugeskr Laeger. 2006 Sep 25;168(39):3314-6. Ugeskr Laeger. 2006. PMID: 17032596 Danish.
-
Treatment of Stage 4 Flatfoot.Foot Ankle Clin. 2020 Jun;25(2):269-280. doi: 10.1016/j.fcl.2020.02.002. Epub 2020 Mar 23. Foot Ankle Clin. 2020. PMID: 32381314 Review.
-
Acquired flatfoot deformity secondary to dysfunction of the tibialis posterior tendon.Acta Orthop Belg. 2003 Jun;69(3):211-21. Acta Orthop Belg. 2003. PMID: 12879702 Review. No abstract available.
-
[Posterior tibial insufficiency].Ugeskr Laeger. 2006 Nov 20;168(47):4113. Ugeskr Laeger. 2006. PMID: 17144002 Danish. No abstract available.
-
[Acquired adult flatfoot deformity: a pragmatic approach].Rev Med Suisse. 2007 Dec 19;3(138):2892-4, 2896-8. Rev Med Suisse. 2007. PMID: 18277765 Review. French.
Cited by
-
Flatfoot diagnosis by a unique bimodal distribution of footprint index in children.PLoS One. 2014 Dec 31;9(12):e115808. doi: 10.1371/journal.pone.0115808. eCollection 2014. PLoS One. 2014. PMID: 25551228 Free PMC article.
-
Current and future advances in practice: mechanical foot pain.Rheumatol Adv Pract. 2023 Oct 31;7(3):rkad081. doi: 10.1093/rap/rkad081. eCollection 2023. Rheumatol Adv Pract. 2023. PMID: 38091412 Free PMC article. Review.
-
The horizontal calcaneofibular ligament: a sign of hindfoot valgus on ankle MRI.Skeletal Radiol. 2020 May;49(5):739-746. doi: 10.1007/s00256-019-03347-1. Epub 2019 Dec 6. Skeletal Radiol. 2020. PMID: 31811347
-
Childhood obesity and its impact on the characteristics of gait stance phases: a cross-sectional study.Eur J Pediatr. 2024 Jan;183(1):123-134. doi: 10.1007/s00431-023-05268-7. Epub 2023 Oct 16. Eur J Pediatr. 2024. PMID: 37843611
-
Self-reported social and activity restrictions accompany local impairments in posterior tibial tendon dysfunction: a systematic review.J Foot Ankle Res. 2018 Aug 30;11:49. doi: 10.1186/s13047-018-0292-z. eCollection 2018. J Foot Ankle Res. 2018. PMID: 30186369 Free PMC article.
References
-
- Mann RA. Acquired flatfoot in adults. Clin Orthop Rel Res 1983;181: 46-51. - PubMed
-
- Johnson KA. Tibialis posterior tendon rupture. Clin Orthop Rel Res 1983;177: 140-7. - PubMed
-
- Haddad FS, Berry G, Singh D, Angel J. Tibialis posterior tendonitis: the forgotten epidemic. Presented at the British Orthopaedic Association, September 1999. J Bone Joint Surg 2000;82B(suppl 1): 80.
-
- Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Non-operative treatment of posterior tibial tendon dysfunction. Foot Ankle Internat 1996;17: 736-41. - PubMed
-
- Kohls-Gatzoulis JA, Singh D. Tibialis posterior dysfunction as a cause of flatfeet in elderly patients. Foot 2004;14: 207-9.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources