

Inhaling to mitigate exhaled bioaerosols
- PMID: 15583121
- PMCID: PMC536048
- DOI: 10.1073/pnas.0408159101
Inhaling to mitigate exhaled bioaerosols
Abstract
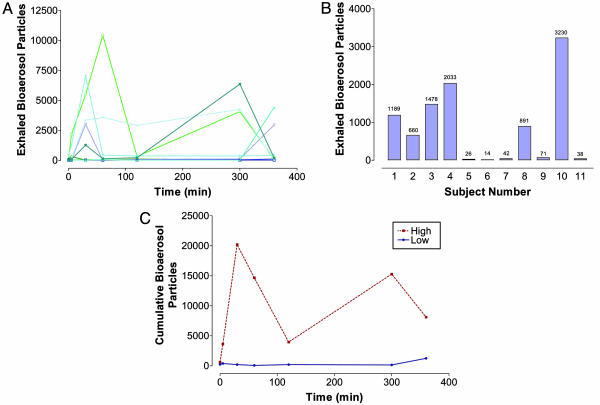
Humans commonly exhale aerosols comprised of small droplets of airway-lining fluid during normal breathing. These "exhaled bioaerosols" may carry airborne pathogens and thereby magnify the spread of certain infectious diseases, such as influenza, tuberculosis, and severe acute respiratory syndrome. We hypothesize that, by altering lung airway surface properties through an inhaled nontoxic aerosol, we might substantially diminish the number of exhaled bioaerosol droplets and thereby provide a simple means to potentially mitigate the spread of airborne infectious disease independently of the identity of the airborne pathogen or the nature of any specific therapy. We find that some normal human subjects expire many more bioaerosol particles than other individuals during quiet breathing and therefore bear the burden of production of exhaled bioaerosols. Administering nebulized isotonic saline to these "high-producer" individuals diminishes the number of exhaled bioaerosol particles expired by 72.10 +/- 8.19% for up to 6 h. In vitro and in vivo experiments with saline and surfactants suggest that the mechanism of action of the nebulized saline relates to modification of the physical properties of the airway-lining fluid, notably surface tension.
Figures
References
-
- Roy, C. J. & Milton, D. K. (2004) N. Engl. J. Med. 350, 1710–1712. - PubMed
-
- Sattar, S. A. & Ijaz, M. K. (1987) in CRC Critical Reviews in Environmental Control, ed. Logan, T. (CRC, Philadelphia), pp. 89–131.
-
- Riley, E. C., Murphy, G. & Riley, R. L. (1978) Am. J. Epidemiol. 107, 421–432. - PubMed
-
- Frankova, V. (1975) Acta Virol. 19, 35–40. - PubMed
-
- Harmory, B. H., Couch, R. B., Douglas, R. G. J., Black, S. H. & Knight, V. (1972) Proc. Soc. Exp. Biol. Med. 139, 890–893. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
