

Accuracy of screening mammography interpretation by characteristics of radiologists
- PMID: 15601640
- PMCID: PMC3143032
- DOI: 10.1093/jnci/djh333
Accuracy of screening mammography interpretation by characteristics of radiologists
Abstract
Background: Radiologists differ in their ability to interpret screening mammograms accurately. We investigated the relationship of radiologist characteristics to actual performance from 1996 to 2001.
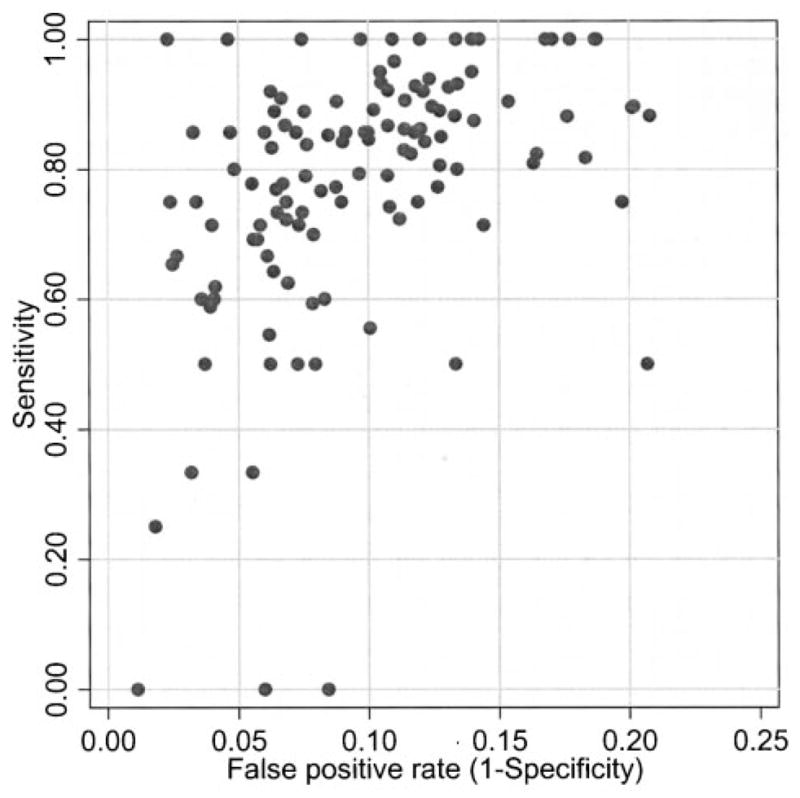
Methods: Screening mammograms (n = 469,512) interpreted by 124 radiologists were linked to cancer outcome data. The radiologists completed a survey that included questions on demographics, malpractice concerns, years of experience interpreting mammograms, and the number of mammograms read annually. We used receiver operating characteristics (ROC) analysis to analyze variables associated with sensitivity, specificity, and the combination of the two, adjusting for patient variables that affect performance. All P values are two-sided.
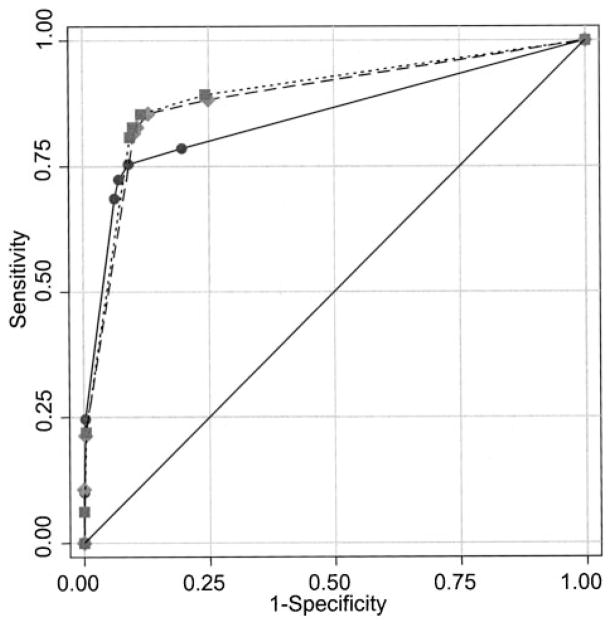
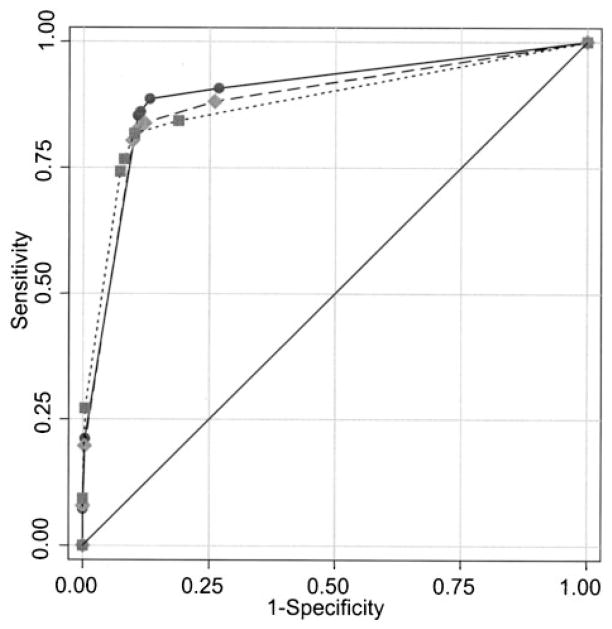
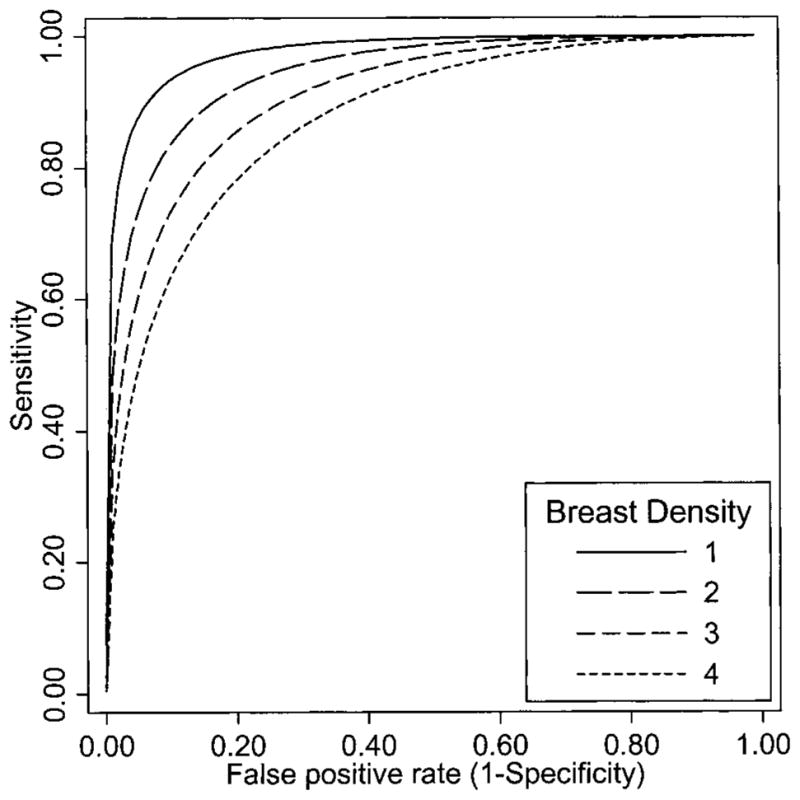
Results: Within 1 year of the mammogram, 2402 breast cancers were identified. Relative to low annual interpretive volume (< or =1000 mammograms), greater interpretive volume was associated with higher sensitivity (P = .001; odds ratio [OR] for moderate volume [1001-2000] = 1.68, 95% CI = 1.18 to 2.39; OR for high volume [>2000] = 1.89, 95% CI = 1.36 to 2.63). Specificity decreased with volume (OR for 1001-2000 = 0.65, 95% CI = 0.52 to 0.83; OR for more than 2000 = 0.76, 95% CI = 0.60 to 0.96), compared with 1000 or less (P = .002). Greater number of years of experience interpreting mammograms was associated with lower sensitivity (P = .001), but higher specificity (P = .003). ROC analysis using the ordinal BI-RADS interpretation showed an association between accuracy and both previous mammographic history (P = .012) and breast density (P<.001). No association was observed between accuracy and years interpreting mammograms (P = .34) or mammography volume (P = .94), after adjusting for variables that affect the threshold for calling a mammogram positive.
Conclusions: We found no evidence that greater volume or experience at interpreting mammograms is associated with better performance. However, they may affect sensitivity and specificity, possibly by determining the threshold for calling a mammogram positive. Increasing volume requirements is unlikely to improve overall mammography performance.
Figures
Comment in
-
Re: Accuracy of screening mammography interpretation by characteristics of radiologists.J Natl Cancer Inst. 2005 Jun 15;97(12):936. doi: 10.1093/jnci/dji156. J Natl Cancer Inst. 2005. PMID: 15956657 No abstract available.
References
-
- Humphrey LL, Helfand M, Chan B, Woolf SH. Breast Cancer Screening: A Summary of the Evidence for the United States Preventive Services Task Force. Ann Intern Med. 2002;137:347–60. - PubMed
-
- United States Preventive Services Task Force. Summaries for patients. Screening for breast cancer: recommendations from the United States Preventive Services Task Force. Ann Intern Med. 2002;137:I47. - PubMed
-
- Zapka JG, Taplin SH, Solberg LI, Manos MM. A framework for improving the quality of cancer care: the case of breast and cervical cancer screening. Cancer Epidemiol Biomarkers Prev. 2003;12:4–13. - PubMed
-
- Elmore JG, Wells CK, Lee CH, Howard DH, Feinstein AR. Variability in radiologists’ interpretations of mammograms. N Engl J Med. 1994;331:1493–9. - PubMed
-
- Beam CA, Layde PM, Sullivan DC. Variability in the interpretation of screening mammograms by US radiologists. Arch Intern Med. 1996;156:209–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
