

Acute improvement of atrial mechanical stunning after electrical cardioversion of persistent atrial fibrillation: comparison between biatrial and single atrial pacing
- PMID: 15604336
- PMCID: PMC1768638
- DOI: 10.1136/hrt.2003.032334
Acute improvement of atrial mechanical stunning after electrical cardioversion of persistent atrial fibrillation: comparison between biatrial and single atrial pacing
Abstract
Objective: To evaluate the acute effects of atrial pacing at different pacing sites on mechanical stunning after cardioversion of atrial fibrillation (AF).
Setting: Tertiary referral centre.
Patients: 20 patients with persistent AF were studied.
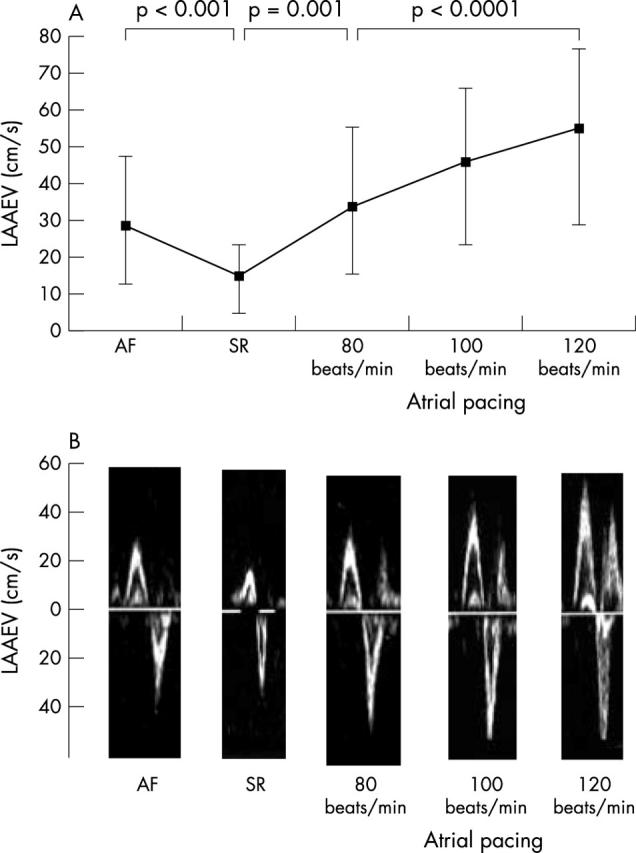
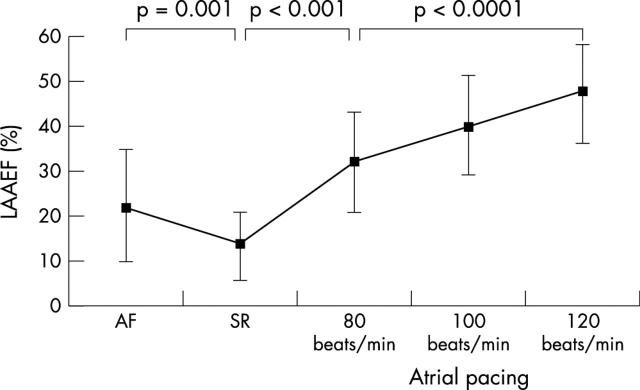
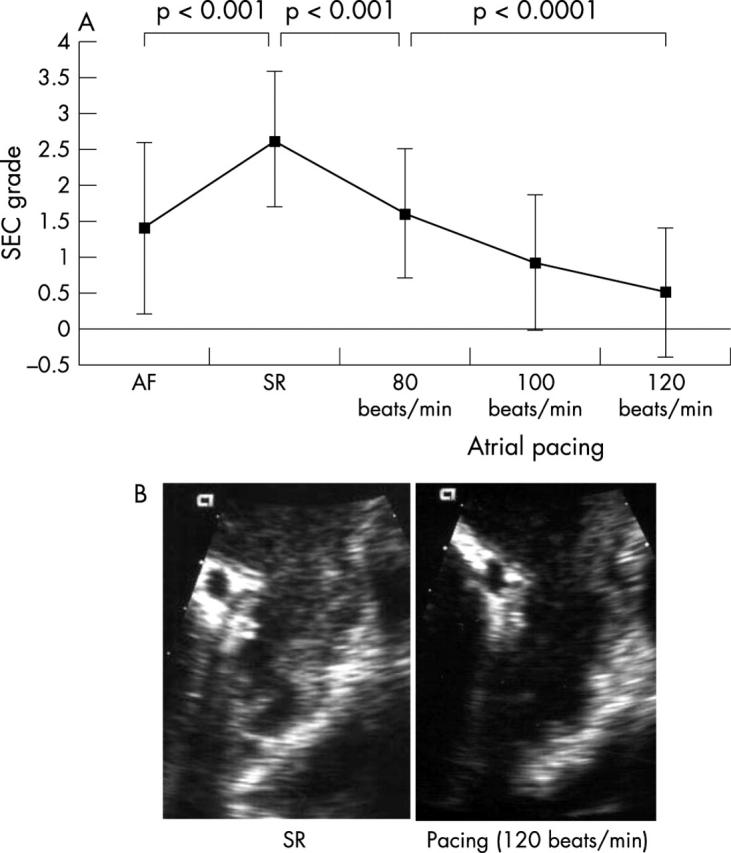
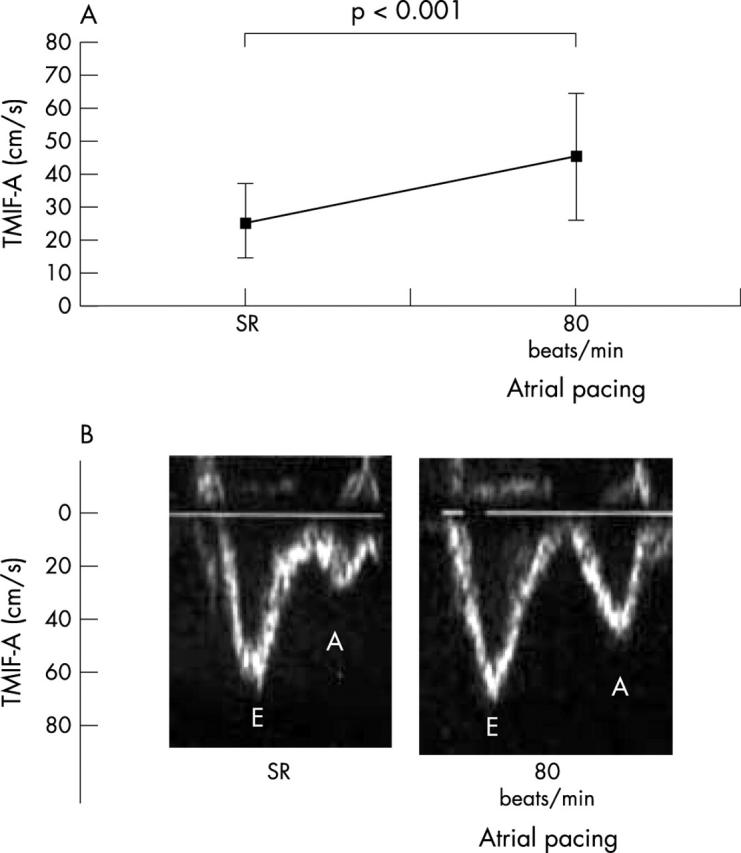
Interventions: Spontaneous echo contrast (SEC), left atrial appendage emptying velocity (LAAEV), and left atrial appendage emptying fraction (LAAEF) were assessed by transoesophageal echocardiography (TOE) during AF, after conversion to sinus rhythm, and during atrial pacing from the right atrial appendage, left lateral atrium, and both atria simultaneously. Transmitral inflow velocity of the atrial wave (TMIF-A) by TOE and the maximum P wave duration in 12 lead ECG were also measured during sinus rhythm and atrial pacing.
Main outcome measures: Comparison of atrial mechanical function and P wave duration in 12 lead ECG during atrial pacing from different sites after cardioversion of AF.
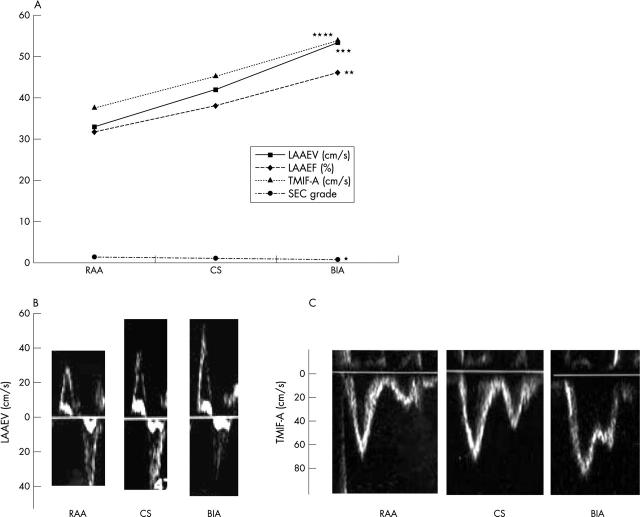
Results: Compared with sinus rhythm, atrial pacing at 80 beats/min increased LAAEV from mean (SD) 14.6 (10.1) to 33.4 (19.8) cm/s (p = 0.001), LAAEF from 13.8 (8.5) to 32.1 (11.2)% (p < 0.001), and TMIF-A from 24.6 (11.9) to 45.6 (21.0) cm/s (p < 0.001) and reduced SEC grade from 2.6 (1.0) to 1.6 (0.9) (p < 0.001). These effects had a positive force-frequency relation. Biatrial pacing produced the shortest P wave duration and resulted in the most significant improvement in atrial function (LAAEV, 33.2 (19.3) v 53.7 (23.9) cm/s, p = 0.0001; LAAEF, 31.9 (11.1) v 46.2 (12.6)%, p < 0.0001; TMIF-A, 37.7 (18.3) v 54.1 (21.2) cm/s, p < 0.001; SEC grade, 1.4 (1.1) v 0.8 (0.9), p = 0.001, right atrial appendage versus biatrial pacing).
Conclusions: Atrial pacing at increased rates can improve atrial mechanical function after cardioversion of persistent AF. Biatrial pacing may be the most effective technique to reverse atrial mechanical stunning.
Figures
Similar articles
-
Reversal of atrial mechanical dysfunction after cardioversion of atrial fibrillation: implications for the mechanisms of tachycardia-mediated atrial cardiomyopathy.Circulation. 2003 Oct 21;108(16):1976-84. doi: 10.1161/01.CIR.0000091408.45747.04. Epub 2003 Oct 13. Circulation. 2003. PMID: 14557372 Clinical Trial.
-
Left atrial mechanical function after brief duration atrial fibrillation.J Am Coll Cardiol. 1999 Feb;33(2):342-9. doi: 10.1016/s0735-1097(98)00585-3. J Am Coll Cardiol. 1999. PMID: 9973013
-
Stunning of the left atrium after conversion of atrial fibrillation: predictor for maintenance of sinus rhythm?Echocardiography. 2005 May;22(5):402-7. doi: 10.1111/j.1540-8175.2005.03167.x. Echocardiography. 2005. PMID: 15901291
-
Transient atrial mechanical dysfunction (stunning) after cardioversion of atrial fibrillation and flutter.Am Heart J. 2002 Jul;144(1):11-22. doi: 10.1067/mhj.2002.123113. Am Heart J. 2002. PMID: 12094183 Review.
-
Atrial stunning: determinants and cellular mechanisms.Am Heart J. 2003 May;145(5):787-94. doi: 10.1016/S0002-8703(03)00086-3. Am Heart J. 2003. PMID: 12766734 Review.
Cited by
-
Cardiac hemodynamics and proinflammatory cytokines during biatrial and right atrial appendage pacing in patients with interatrial block.J Interv Card Electrophysiol. 2013 Aug;37(2):147-54. doi: 10.1007/s10840-013-9792-8. Epub 2013 Apr 28. J Interv Card Electrophysiol. 2013. PMID: 23625090 Free PMC article. Clinical Trial.
References
-
- Grimm RA, Stewart WJ, Maloney JD, et al. Impact of electrical cardioversion for atrial fibrillation on left atrial appendage function and spontaneous echo contrast: characterization by simultaneous transesophageal echocardiography. J Am Coll Cardiol 1993;22:1359–66. - PubMed
-
- Fatkin D, Kuchar DL, Thorburn CW, et al. Transesophageal echocardiography before and during direct current cardioversion of atrial fibrillation: evidence for “atrial stunning” as a mechanism of thromboembolic complications. J Am Coll Cardiol 1994;23:307–16. - PubMed
-
- Grimm RA, Leung DY, Black IW, et al. Left atrial appendage “stunning” after spontaneous conversion of atrial fibrillation demonstrated by transesophageal Doppler echocardiography. Am Heart J 1995;130:174–6. - PubMed
-
- Antonielli E, Pizzuti A, Bassignana A, et al. Transesophageal echocardiographic evidence of more pronounced left atrial stunning after chemical (propafenone) rather than electrical attempts at cardioversion from atrial fibrillation. Am J Cardiol 1999;84:1092–6. - PubMed
-
- Manning WJ, Leeman DE, Gotch PJ, et al. Pulsed Doppler evaluation of atrial mechanical function after electrical cardioversion of atrial fibrillation. J Am Coll Cardiol 1989;13:617–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical